CD8+ T cell
Immune-Oncology Assays
- 2D/ 3D Tumour Killing Assay (panel of tumour cells available)
- Antigen-specific CTL-CEFT (phenotype, proliferation, degranulation)
- MART-1 specific CTL- cytotoxicity
- T cell exhaustion
Autoimmunity Assays
- Activation
- Proliferation and function
Assays
3D immune mediated Tumour Killing Models: Tools for screening immune or tumour targeted therapeutics
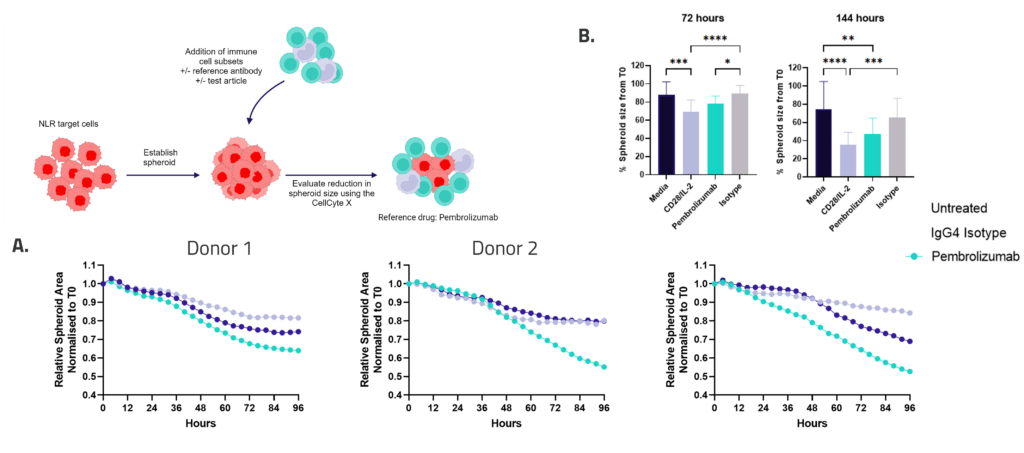
Figure 1: SKOV-3 NLR tumour cells were seeded into 96 well plates, PBMC were added once spheroids were established in the presence of Pembrolizumab or IgG4 control or vehicle (untreated) and imaged every 4 hours for 96 hours using the CellCyte X. Relative spheroid area (%) was measured (A). AUC statistics were calculated using GraphPad Prism v9.5.0
Enzyme-Linked Immuno Spot (ELISpot) enables quantification of rare immune cells in response to antigenic stimulation
ELISpot is a highly sensitive method to test immune modulators, novel vaccine candidates or de-risk immunogenicity testing in an antigen-specific CD4 and/or CD8 T cell assay.
| Condition | Aim |
| No Stimulation | Negative control |
| PMA | Positive control |
| CERI (CMV, EBV, RSV, Influenza) | MHC-I restricted peptide pool to evaluate modulation of CD8+ T-cell memory response |
| CPI (CMV, Parainfluenza, Influenza) | Positive protein antigens to evaluate modulation of CD4+ T-cell memory response |
| CEF (CMV, EBV, Influenza) | MHC-I restricted peptide pool to evaluate modulation of CD8+ T-cell memory response |
| Cyclosporin A (CsA) | Inhibition of immune response |
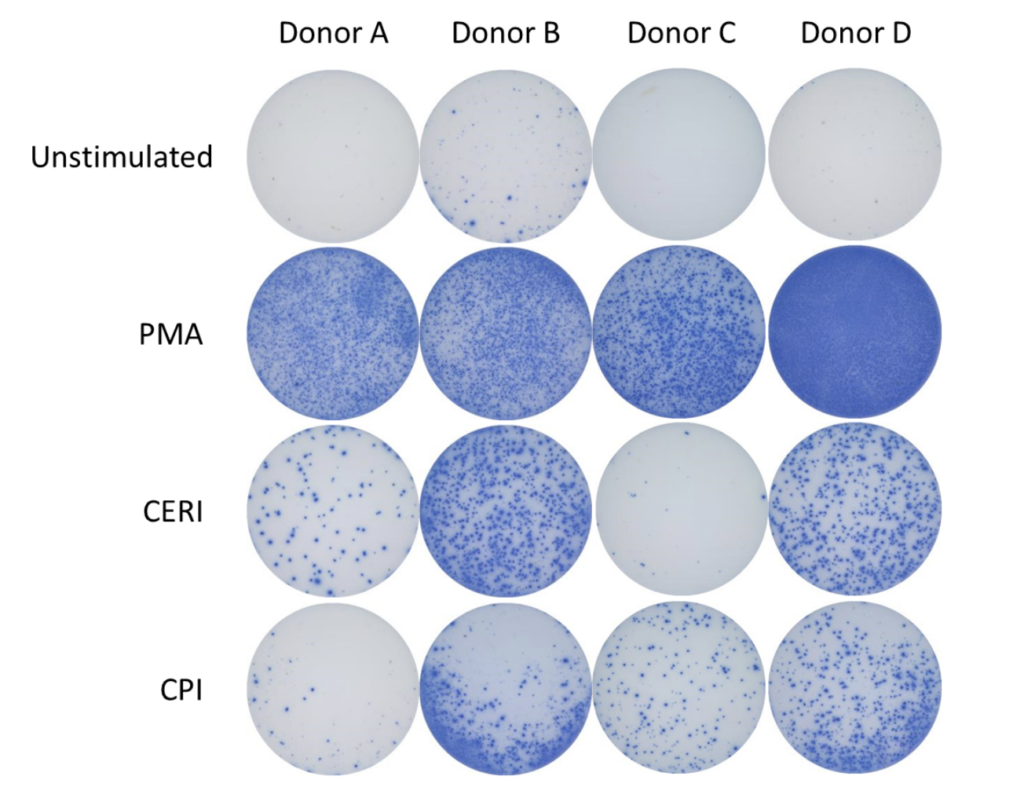
Figure 1: The ELISpot visual image results showing four donors under four conditions: Unstimulated (negative control), stimulated with PMA (positive control), stimulated with CERI, and stimulated with CPI antigens. Each purple spot represents one IFNγ producing cell.
Spot Forming Units (SPU) for IFN-γ per 100,000 PBMC from CERI, CPI and CEF antigens for three donors
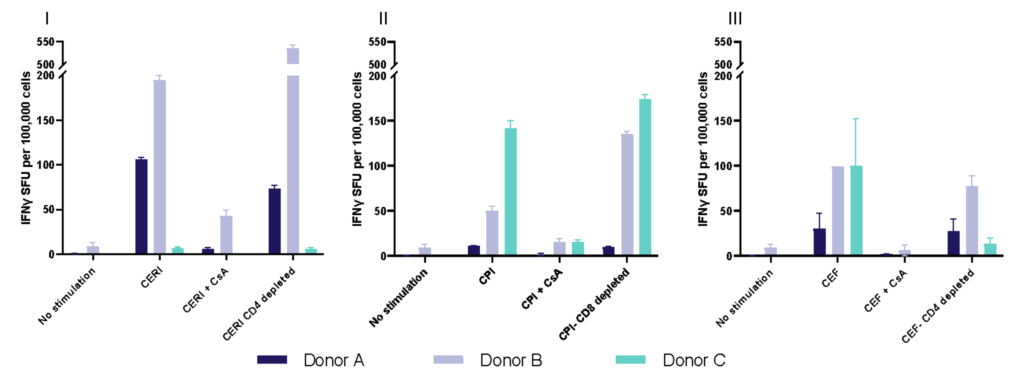
Figure 2: T cell responses from three donors using stimuli, CERI (I), CPI (II) and CEF (III). Expressed as spot forming units per 100,000 donor PBMC. Depletion of CD4 or CD8 T cells demonstrates specificity of response to peptide pools. Each value represents the mean of triplicate wells ±SEM.
I. T cell response to Tetanus Toxoid, Influenza and PPD antigens
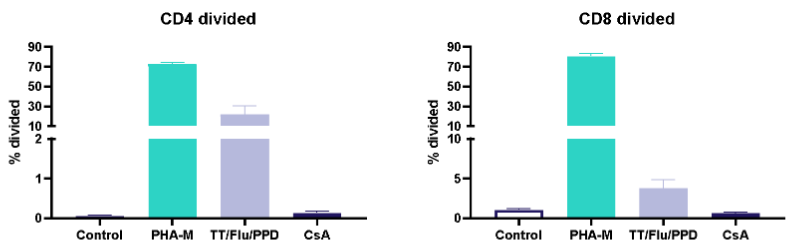
II. Dose response to Influenza antigen
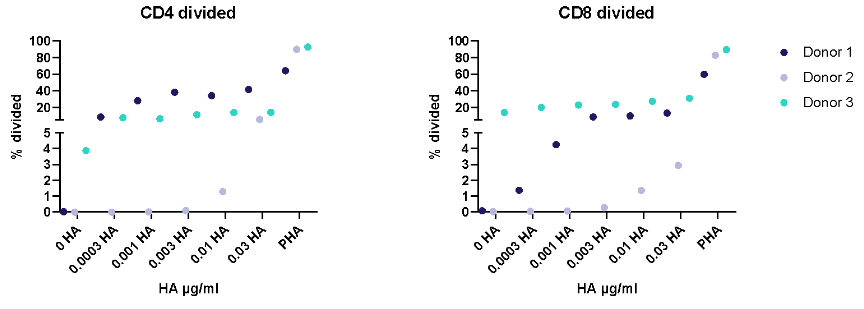
Antigen specific T cells response to a recall antigens. (I) Healthy donors PBMC were stimulated with PHA-M or triple antigen cocktail (Tetanus Toxoid, Influenza and PPD). Cyclosporin was used as a reference treatment. (II) Dose response to Influenza antigen. CD4 and CD8 T cells proliferation was measured by flow cytometry using CTV dilutions.
Natural Killer Cell
Immune-Oncology Assays
- Activation, proliferation and killing (KIR/NKG2D/ ADCC)
- ADCC tumour cells or pathogenic autoreactive immune cells
- CRA-predictive toxicity
Assays
Antibody dependent cell cytotoxicity (ADCC) in a 3D tumour spheroid model
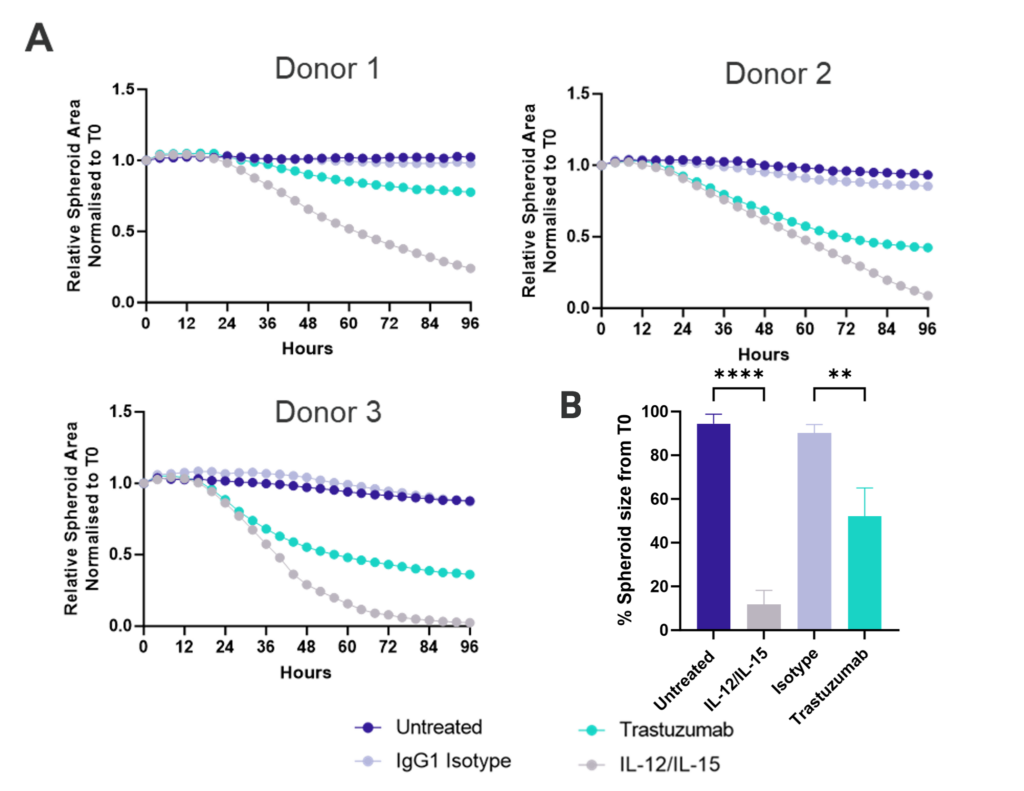
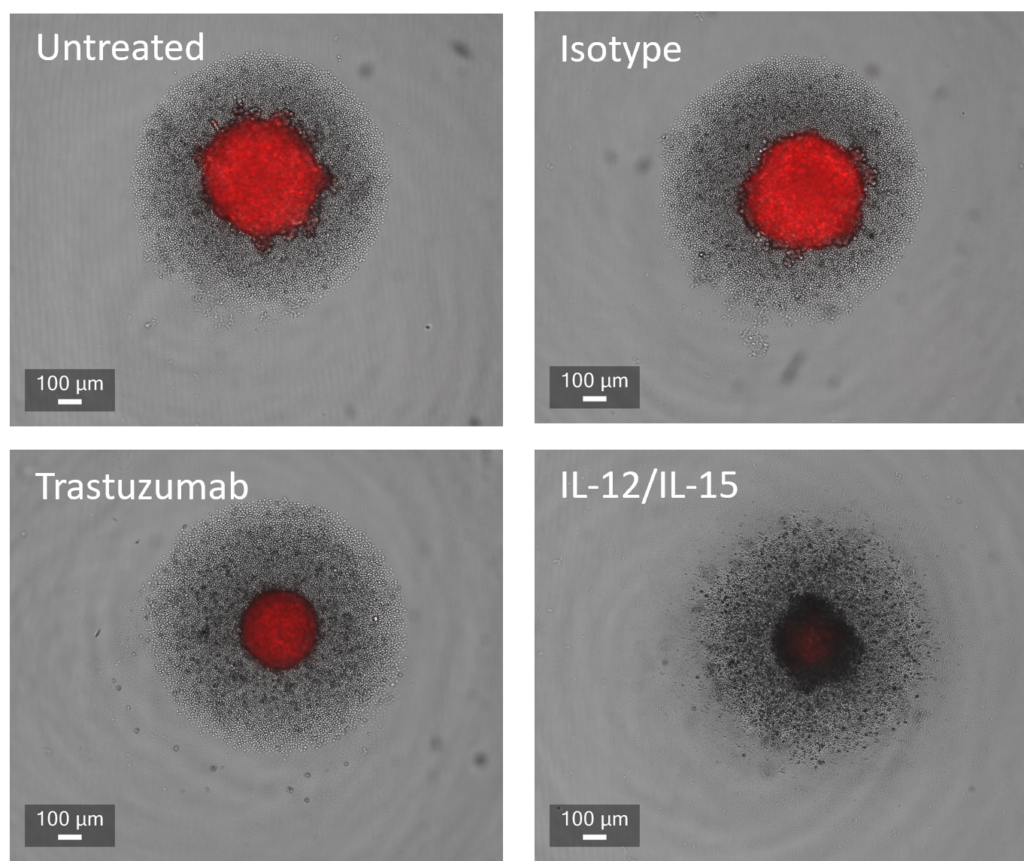
Figure 1: SK-OV-3 NLR cells expressing HER2 were plated were seeded into 96 well plates and once spheroids were established purified NK cells were added to cultures in the presence of Trastuzumab or IgG1 Isotype or IL-12/IL-15 or vehicle (untreated) and imaged every 4 hours for 96 hours using the CellCyte X. Relative spheroid area (%) was measured (A) and the AUC (B) calculated using GraphPad Prism v9.5.0. Line graphs show the mean of triplicate wells and the bar graph shows mean +/- SEM of 9 donors. (C) Representative images from the CellCyte X at 96 hours post NK cell addition to tumour spheroids.
Assessing antibody dependent cell cytotoxicity (ADCC) driving the depletion of pathogenic immune cell subsets
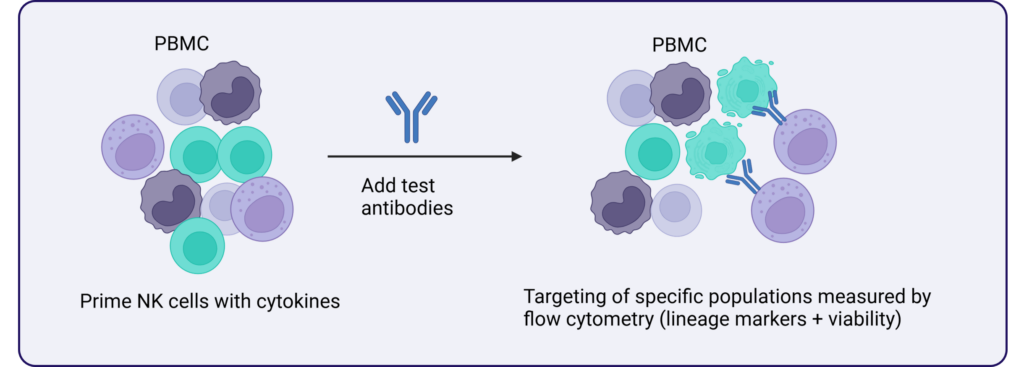
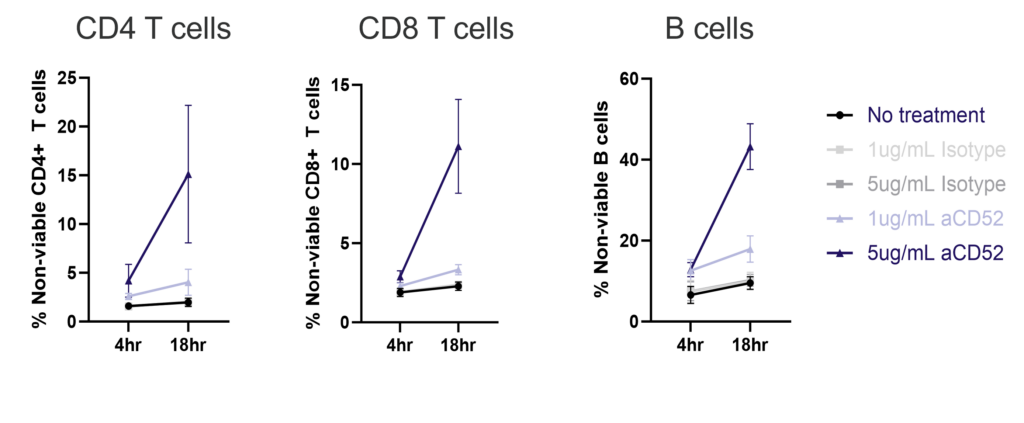
ADCC PBMC assay to test specificity of the immune cell depleting antibody Alemtuzumab. Anti-CD52 antibody (Alemtuzumab) mediates killing via ADCC of CD52 expressing immune cells including T and B cells. The viability of CD4, CD8 and B cells was measured by flow cytometry after 4 and 18h of culture in the presence of an anti-CD52 IgG1 (Alemtuzumab) antibody or isotype at two concentrations. Graphs show mean +/- SEM, n=3 donors.
Macrophage
Immune-Oncology Assays
- ADCP
- MDSC
- M1/M2
- TAM
- Efferocytosis
- Phagocytosis
- Cytokine Release Assay (CRA)-predictive toxicity
Inflammation Assays
- M1/M2 polarisation and function
- Cytokine Release Assay (CRA)-predictive toxicity
Assays
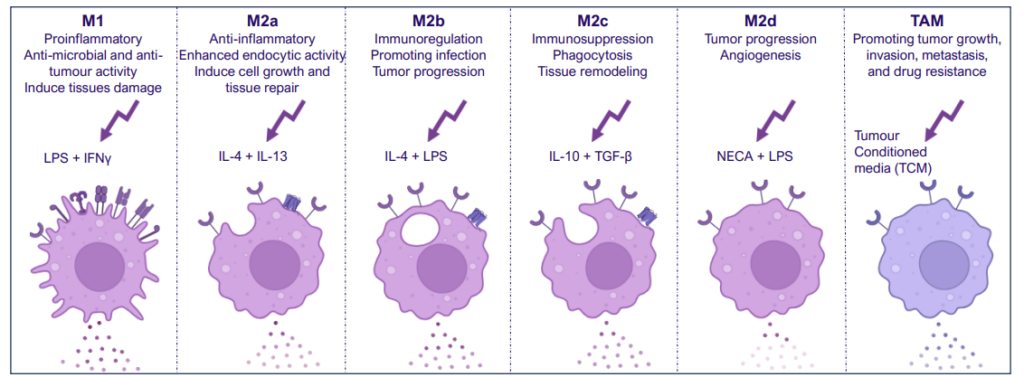
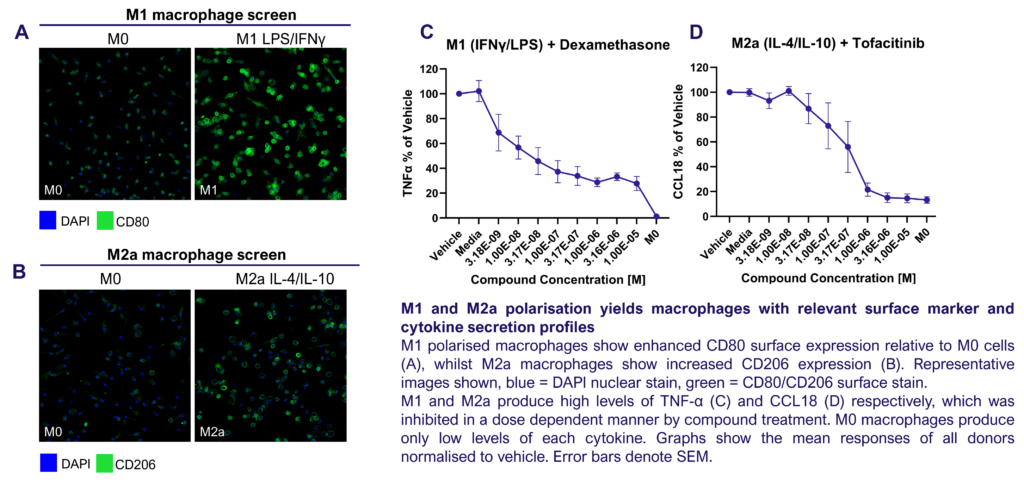
M1/ M2a-d polarisation assay
Monocyte derived macrophages (moMΦ) are differentiated from monocytes isolated from healthy blood donors followed by polarisation into a range of phenotypes M1/ M2a-d and TAM phenotypes using the stimuli described below. Readouts include flow cytometric analysis of surface markers associated with different subsets, production of cytokines and chemokines and ability to phagocytose. Therapeutics can be added at the monocyte to macrophage differentiation phase or polarisation phase to prevent or drive polarisation into a distinct macrophage phenotype.
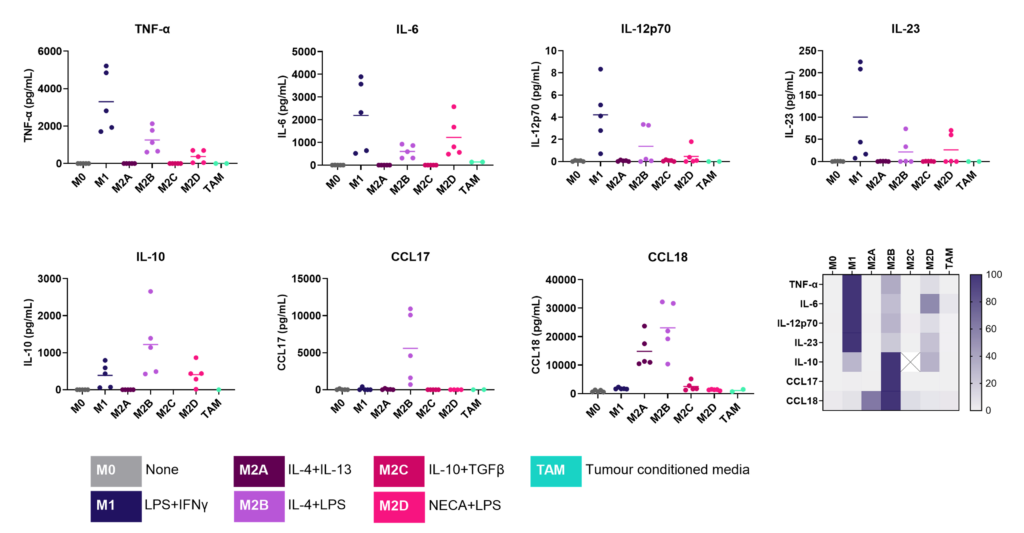

We present a medium-throughput human macrophage assay to screen novel therapeutics that modulate pro-inflammatory M1 (IFNγ/LPS) and anti-inflammatory M2 (IL-4/IL-10) macrophage subsets. Dexamethasone and tofacitinib are used as reference drugs for benchmarking.
Dysregulated macrophage polarisation exacerbates various diseases. Therapeutics that target macrophage re-polarisation could modify the disease state by shifting macrophages to a beneficial phenotype. For example, promoting an inflammatory M1 phenotype could benefit the tumor microenvironment, while fostering an anti-inflammatory phenotype could help in autoimmune and inflammatory diseases.
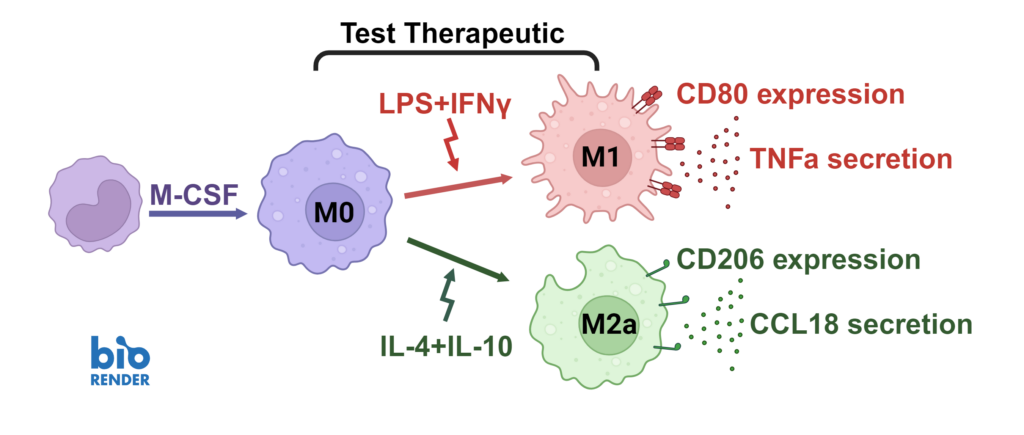
Macrophages were differentiated from monocytes and polarised to M1 or M2a phenotypes following the schema to the left. Polarisation was assessed through CD80 staining and TNFα secretion for M1, and CD206 staining and CCL18 secretion for M2a; staining quantified via HCS analysis. Inhibition of M1 and M2a polarisation was demonstrated using dexamethasone and tofacitinib as reference compounds. Novel therapeutics can be benchmarked against these references.
A THP-1 macrophage cytokine release assay (CRA) can be used to explore modulators of an inflammatory response or “de-risk” any potential unwanted effects of novel therapeutic delivery systems.
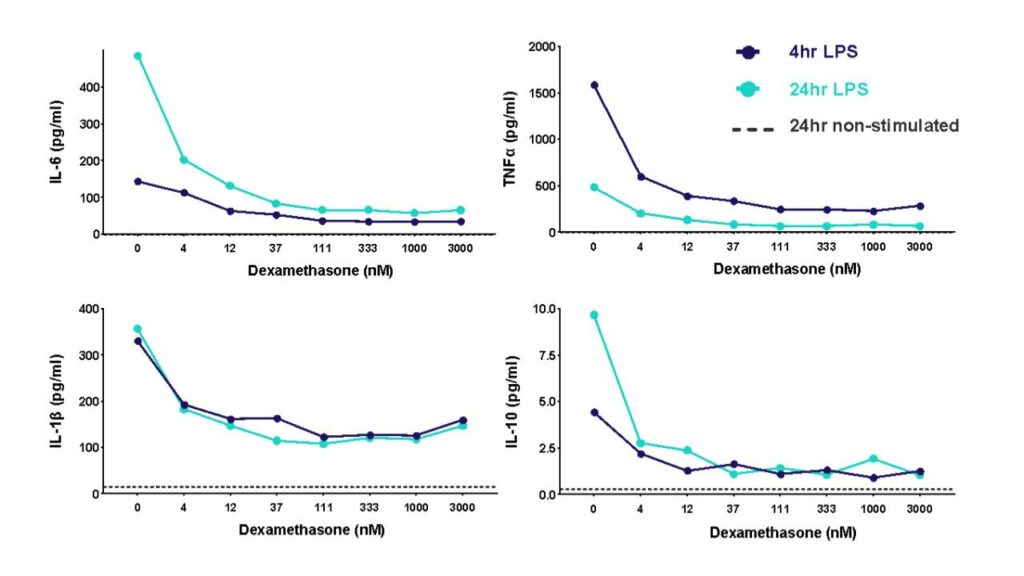
THP-1 cells were differentiated with PMA and then stimulated with LPS to induce cytokine release in the presence of different concentrations of the corticosteroid dexamethasone. Cytokine release was measured at 4h and 24h post LPS stimulation.
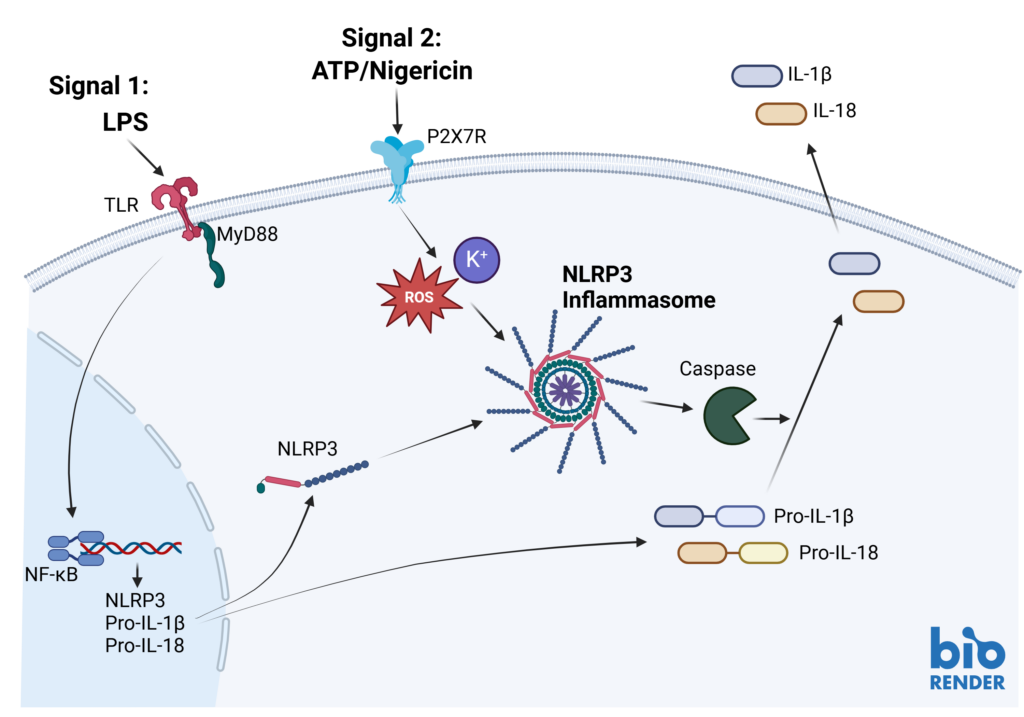
Inflammasome complexes form in response to infection, tissue damage or metabolic imbalances. Once formed the inflammasomes activate Caspase 1 which in turn activated the pro-inflammatory cytokines IL-1β and IL-18. Targeting the inflammasome and the resulting signaling pathways is a useful tool in modulating the immune system.
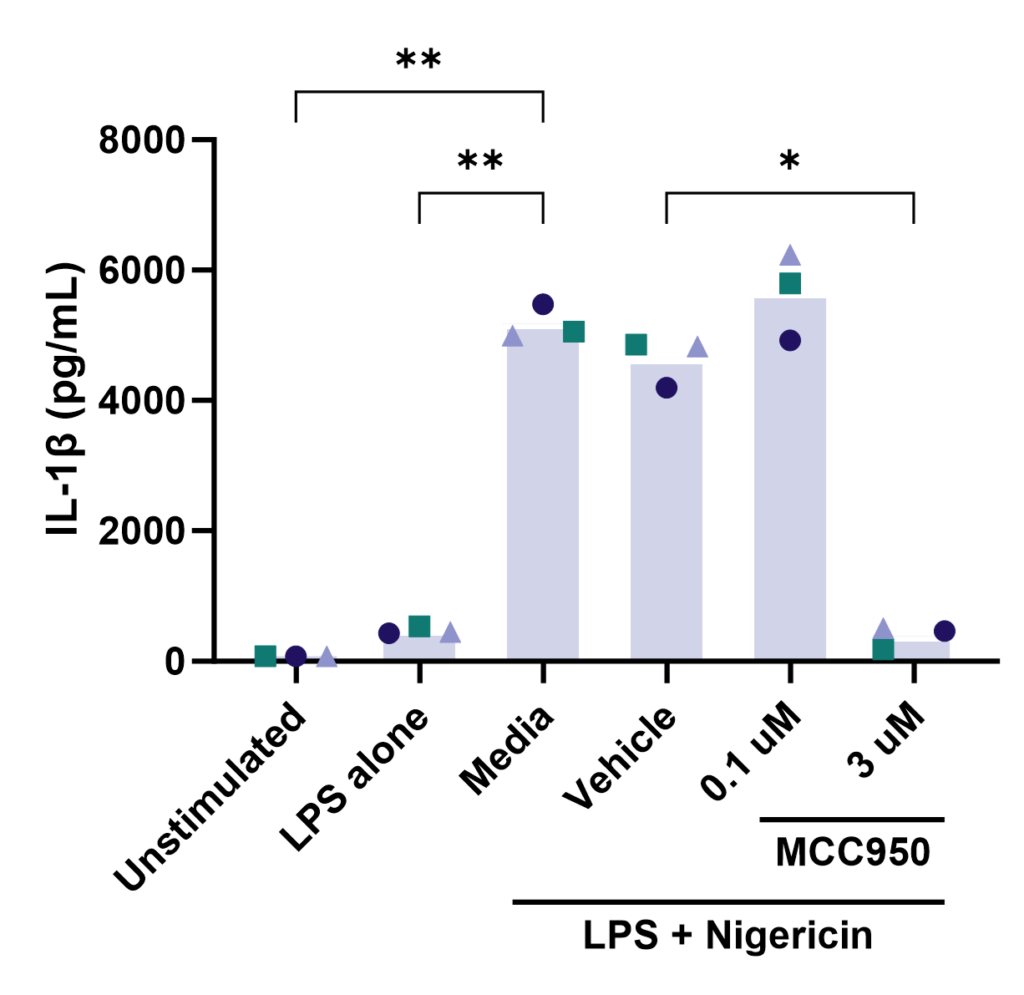
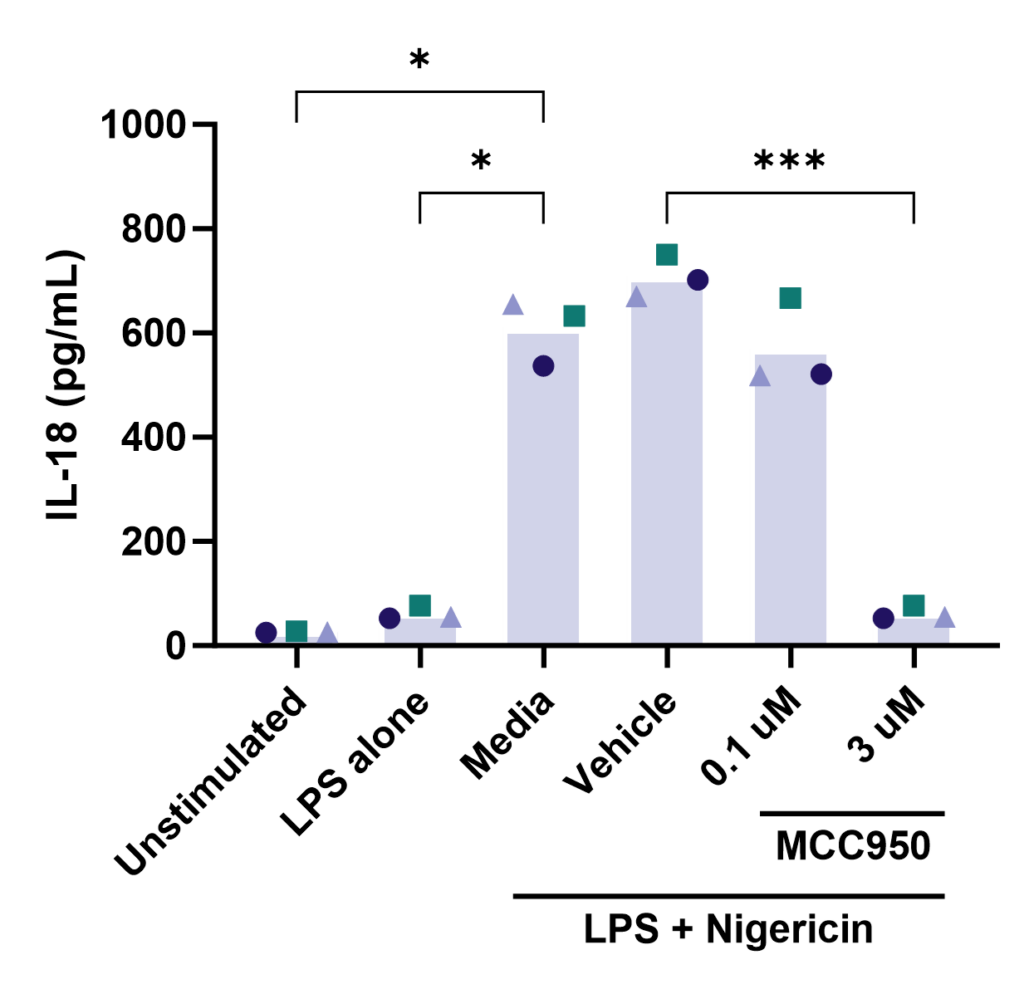
Effect of MCC950 on Inflammasome activation – IL-1β and IL-18. PBMC from three healthy donors were pretreated with MCC950, vehicle (DMSO) or media for 1 hours prior to stimulation with LPS for 4 hours. Nigericin was then added for a further 45 minutes prior to harvest of the cell culture supernatant for quantification of (A) IL-1β and (B) IL-18 by TR-FRET and ELISA respectively. Data points show mean +/- SEM of technical replicates. One-way ANOVA with Dunnett’s multiple comparisons test comparing stimulated (media) to unstimulated, LPS alone, vehicle and MCC950 to vehicle; *<0.05, **<0.01, ***<0.001.
Other formats: PBMC, macrophage subsets, microglia
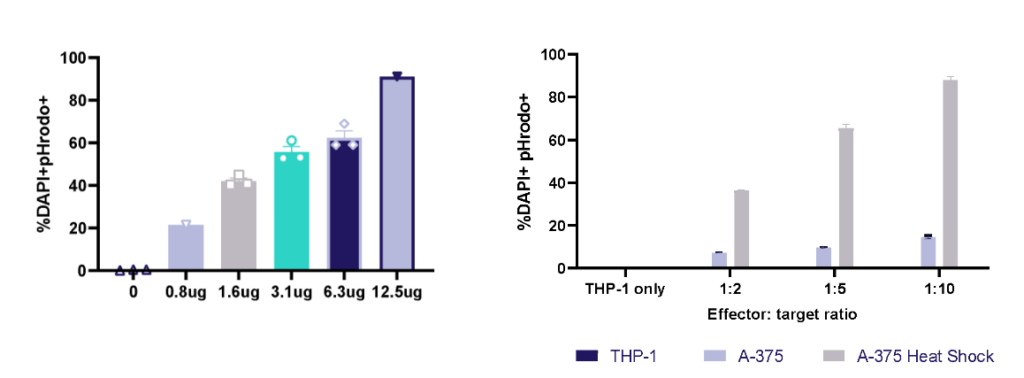
THP-1 macrophage phagocytosis of E.Coli bioparticles and efferocytosis of Heat Shock treated A-375 melanoma tumour cells. THP-1 cells were cultured with E.Coli bioparticles 0-12.5ug/ml; at 1h phagocytosis was evaluated by pHrodo+ cells using flow cytometry. THP-1 cells were cultured with three E:T ratios of A-375 or heat shock treated A-375; at 1h efferocytosis was evaluated by pHrodo+ cells using flow cytometry.
Microglia
Neuro-Inflammation Assays
- iPSC derived Microglia phagocytosis
- iPSC derived Microglia cytokine (Inflammasome) /chemokine release
Assays
Microglia (M) play a role in neuro degeneration by secreting reactive oxygen species (ROS) and pro-inflammatory cytokines, such as Interleukin 1 beta (IL-1β), Interleukin 6 (IL-6) and Tumor Necrosis Factor (TNF-α). Microglial crosstalk with non-neuronal cells shapes their phenotype, either skewing it towards a pro-inflammatory (red arrows) on anti-inflammatory (green arrows) phenotype.

https://doi.org/10.3389/fimmu.2023.1223096


Effect of Dexamethasone on iPSC microglia activation – IL-1β and IL-6. iPSC derived microglia were stimulated with LPS in the presence or absence of Dexamethasone. Cell culture supernatants were harvested and cytokine levels were quantified (A) IL-1β and (B) IL-6 by TR-FRET and ELISA respectively. Data points show mean +/- SEM of technical replicates.
Other formats: microglia stimulation using LPS+ Nigericin, alpha-synuclein
Dendritic Cell
Immune-Oncology Assays
- Antigen uptake and vaccine delivery
- Cross presentation
- Neo-antigen immunogenicity; phenotyping,
Autoimmunity Assays
- Antigen presentation
Assays
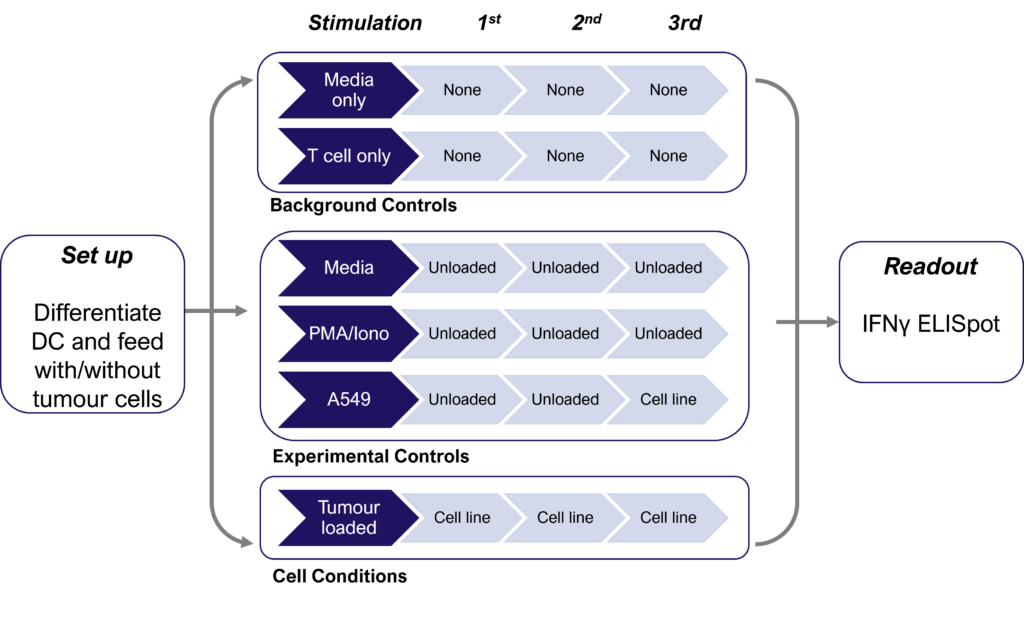
Therapies targeting the modification of tumor cells to increase neoantigen expression and improve immune cell recognition are currently under development. Detecting these subtle changes typically involves several cycles of dendritic cell restimulation of T cells, followed by the sensitive measurement of rare neoantigen-specific T cell responses using IFNγ ELISPOT assays. The schematic below shows the assay design with multiple round of dendritic cell (DC) restimulation to expand rare neoantigen T cell responses.
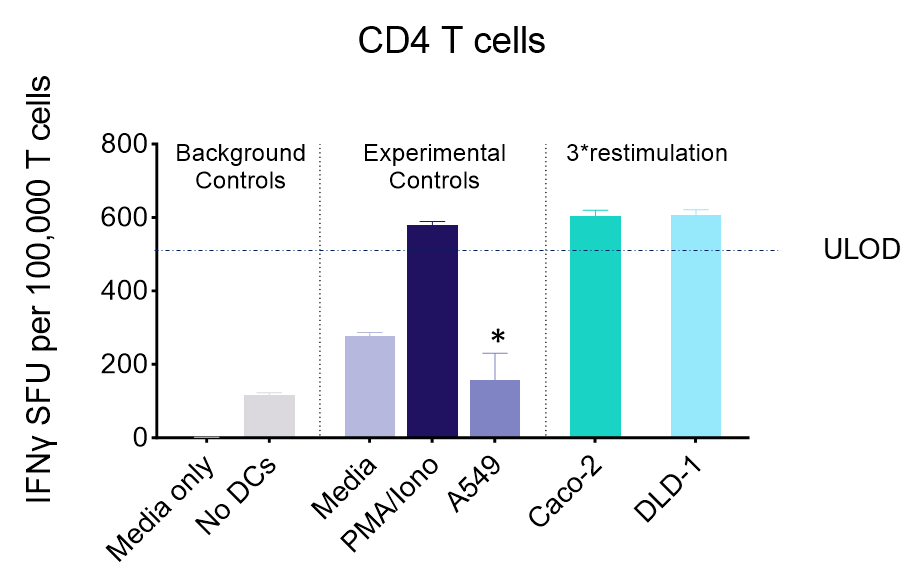
IFNγ release from activated tumour neoantigen-specific CD4 T cells
IFNγ release from activated tumour neoantigen-specific naive CD8 T cells
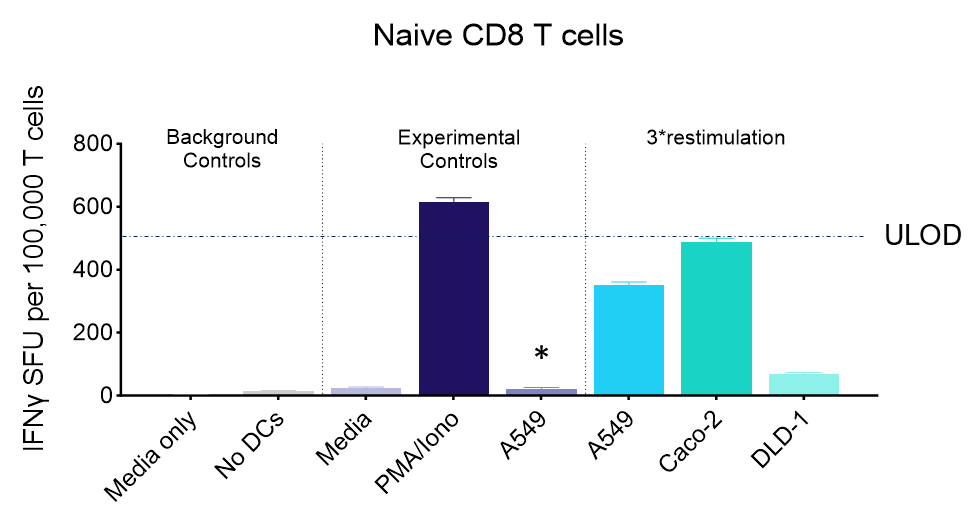
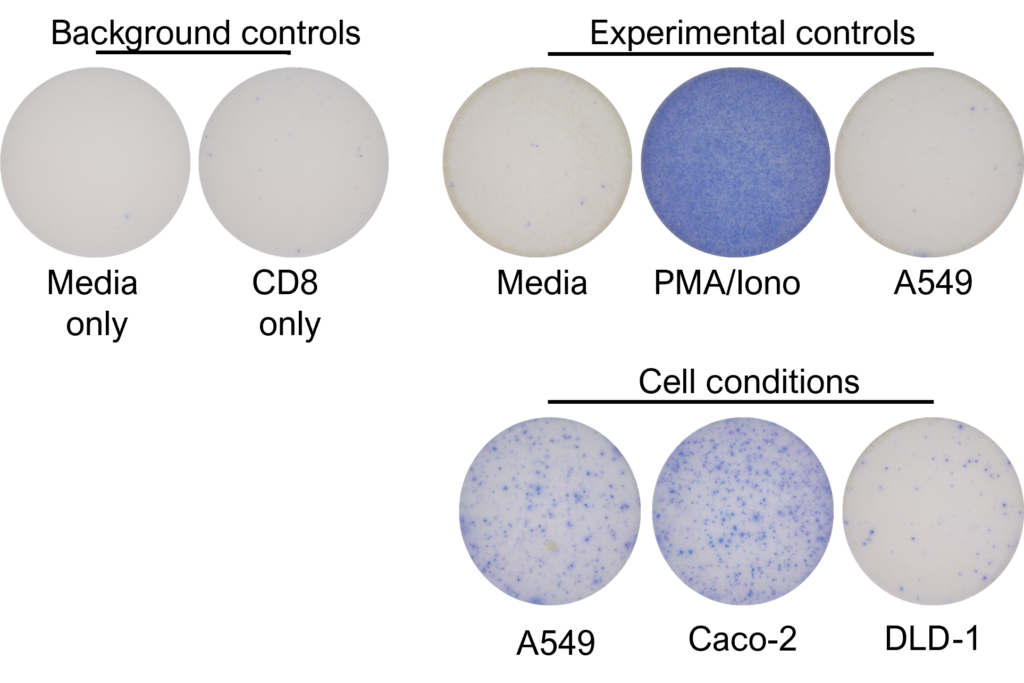
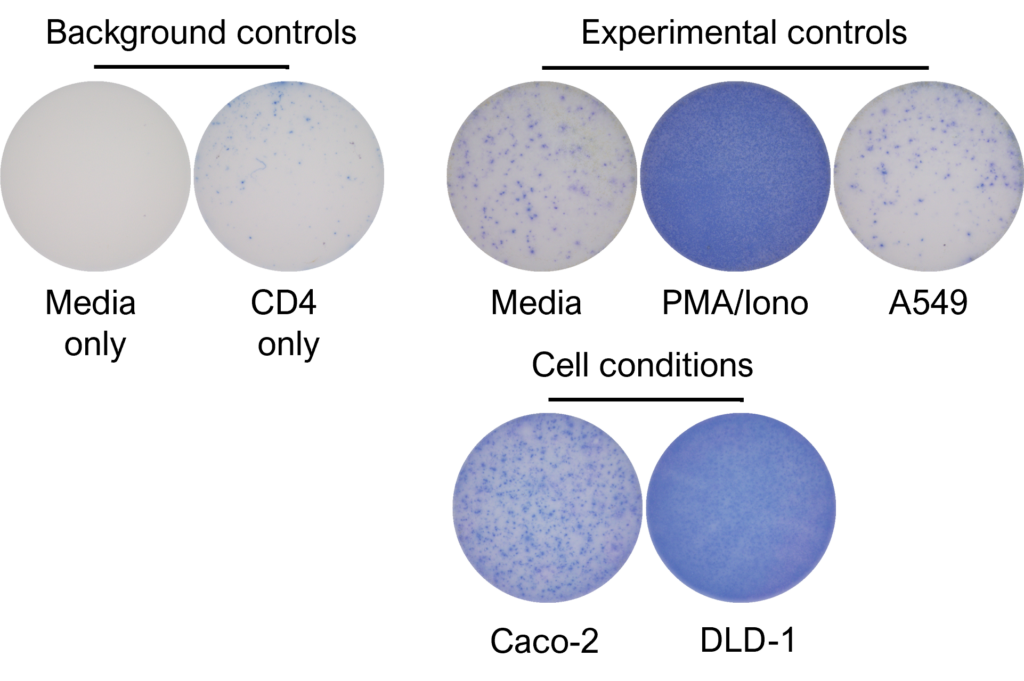
Figures: CD4 or naïve CD8 T cells were co-cultured with unloaded dendritic cells (DC), or with DC loaded with tumour cells that had been previously treated with media or vehicle. Three rounds of stimulation of T cells with DC were performed (* single round of DC stimulation). PMA and ionomycin were added as positive controls during the final round of stimulation. T cell stimulation was assessed by measuring the number of spot forming units (SFU) by IFNγ ELISpot. Media and T cell only wells were included as background controls. Number of SFU per 100,000 plated T cells, with mean of two (experimental controls) or three (all others) replicates ± SEM shown. Representative images of CD4 and naïve CD8 T cell IFNγELISpot. Each blue dot represents one IFNγ-producing T cell. ULOD = Upper Limit of Detection
Neutrophil
Inflammation Assays
- Respiratory Burst (ROS, Phagoburst)
- NETs
- Phagocytosis/trogocytosis
Assays
Neutrophils are armed with a variety of effector mechanisms, they release neutrophil extracellular traps (NETs), comprising of chromatin and antimicrobial proteins which are released via a unique, pro-inflammatory form of cell death called NETosis. Dysregulated NET release can damage the host, contributing to autoimmune diseases such as Systemic Lupus Erythematosus (SLE) by the release of autoantigens. Similarly, dysregulated NET release contributes to diseases such as atherosclerosis, deep vein thrombosis and has been shown to promote cancer progression and metastasis. Modulating neutrophil function is therefore a potential therapeutic intervention.
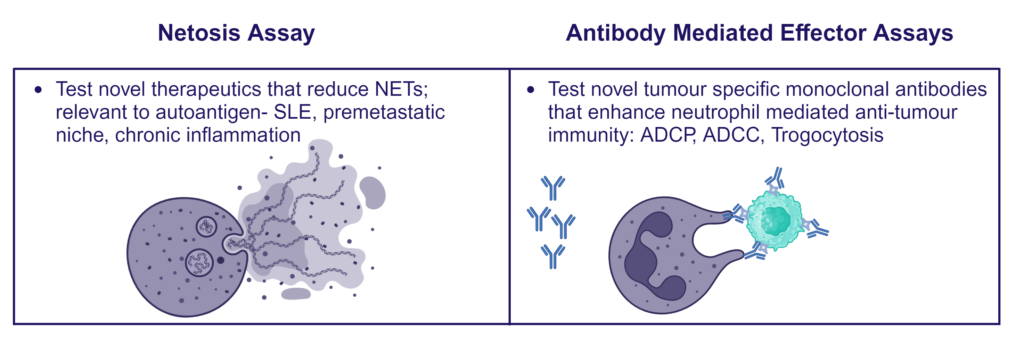
Immune complex-driven NETosis in autoimmune inflammation
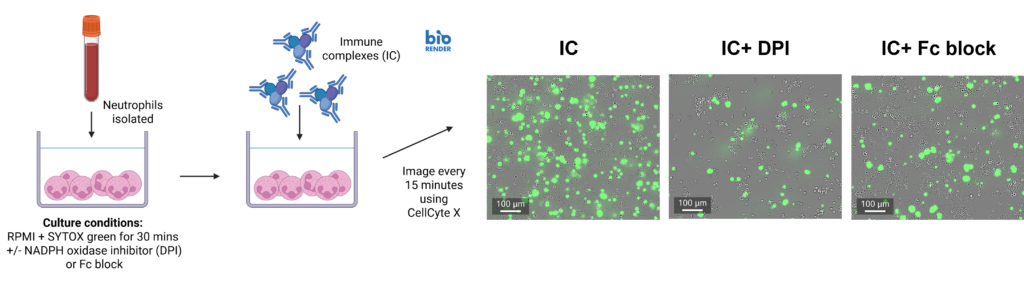
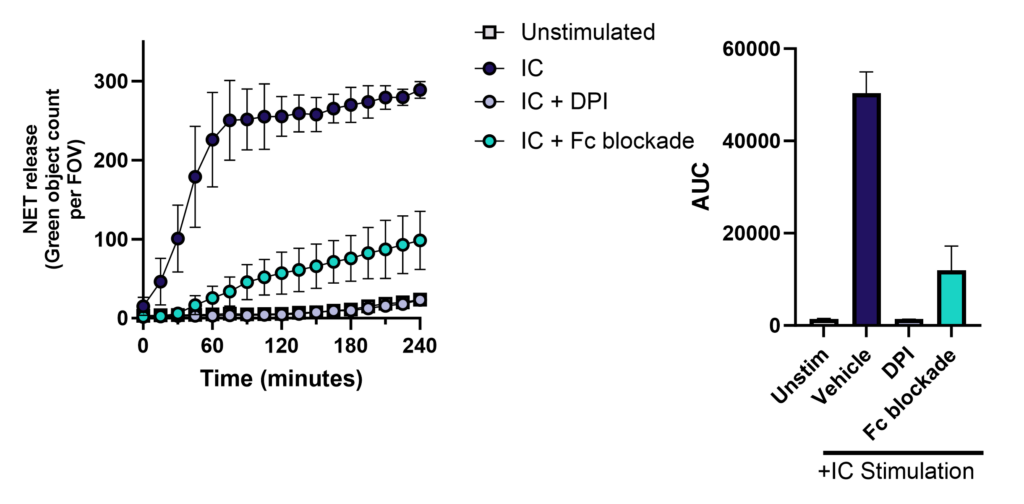
Neutrophils were isolated from fresh blood, cultured with or without NOX2 inhibitor (DPI) or Fc block, and then stimulated with immune complexes (IC) in the presence of SYTOX green to detect NETs. Cells were imaged for green fluorescence (NETs) every 15 minutes for 4 hours. Data shows that NETosis increases in response to stimulation with IC and is inhibited by Fc blockade or DPI.
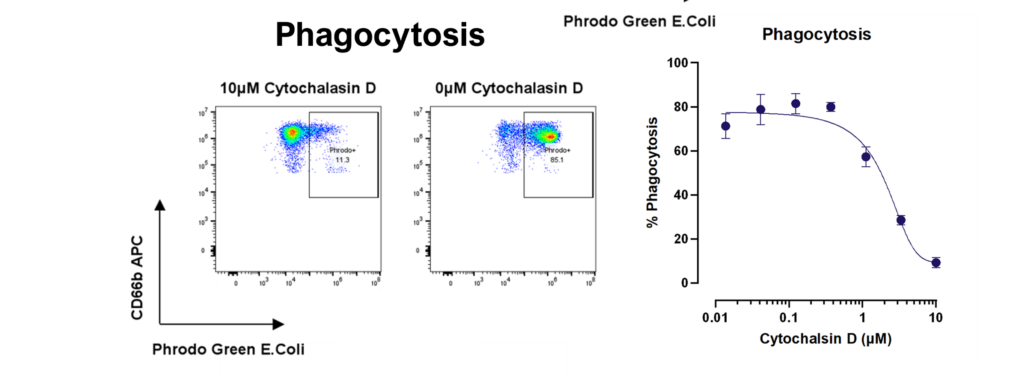
Phagocytosis – Neutrophils were cultured with pHrodo labelled E. coli in the presence or absence of a titration of cytochalasin D and phagocytosis measured by flow cytometry. Phagocytic neutrophils were identified as CD66b+ pHrodo+.
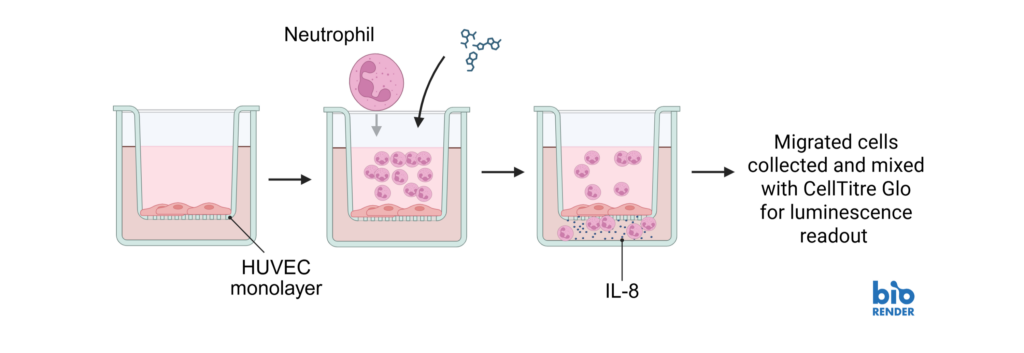
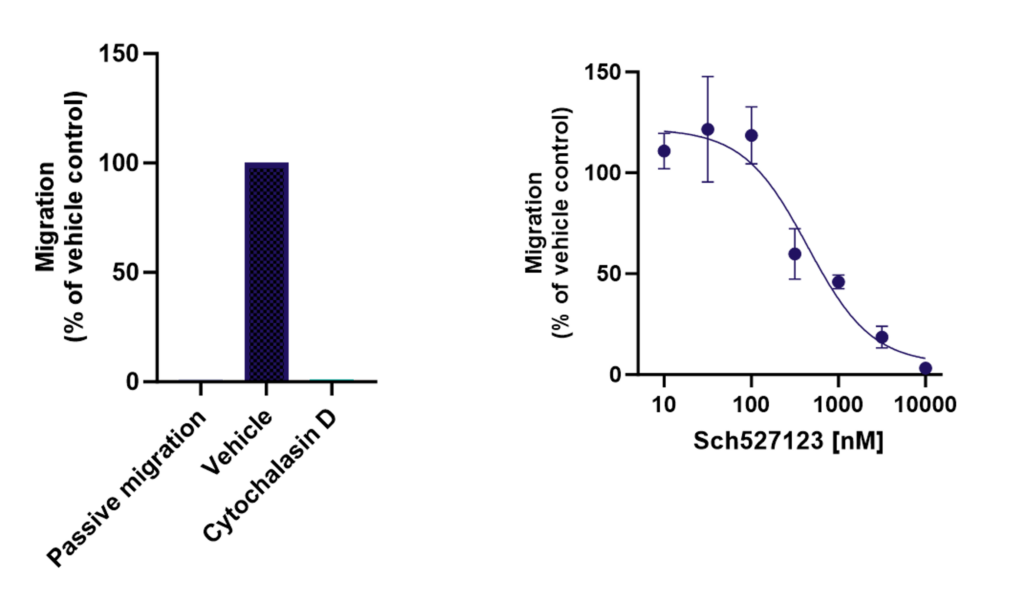
Endothelial cells (HUVEC) were cultured on transwell inserts and confluency confirmed. Neutrophils were isolated from fresh blood and plated on top of the endothelial layer in the presence or absence of CXCR1/2 antagonist (Sch527123), Cytochalasin D, or controls. Chemoattractant IL-8 was added to the lower chamber of the transwell and cells were allowed to migrate before being analysed by luminescence. Sch527123 demonstrated a dose responsive inhibition of neutrophil migration across the endothelial monolayer. Neutrophil migration was inhibited by the positive control, Cytochalasin D.
B cell
Autoimmunity Assays
- Antibody production (Total IgG)
- Memory B cell Antibody Isotypes
- Naïve B cells Isotype switching
- B cell proliferation/activation/cytokine secretion
- Antigen presentation
Assays
Tonsils are a secondary lymphoid tissue rich in B cell subsets and the specialized, anatomically restricted T follicular helper (Tfh) subset of CD4 T cells. Tonsils provide an accessible source of cells for those interested in B cell immunology, Tfh biology and vaccine development. The tonsillar cell re-aggregate model provides functional insight into human germinal center biology, allowing measurement of key features including naive B cell differentiation, plasma cell/plasmablast differentiation, and antibody production.

Figure A. Schematic representation of tonsil re-aggregate model. Cells are seeded at high density in 96 well plates; unstimulated (US) or stimulated with quadrivalent inactivated influenza vaccine (IIV) in the presence of vehicle or reference inhibitors such as Rapamycin. B cell readouts include B cell phenotyping, B cell proliferation and hemagglutinin (HA)-specific IgG by ELISPOT or ELISA.
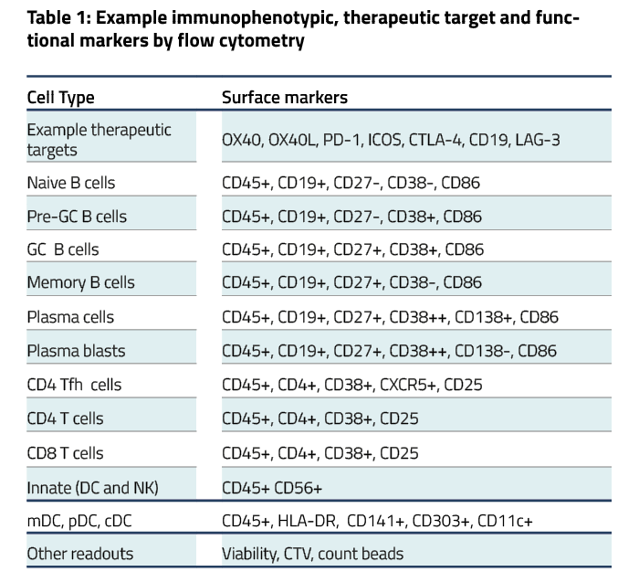
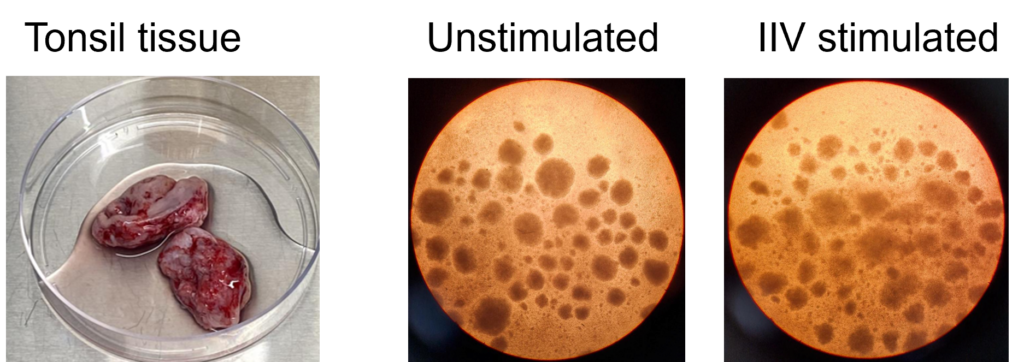
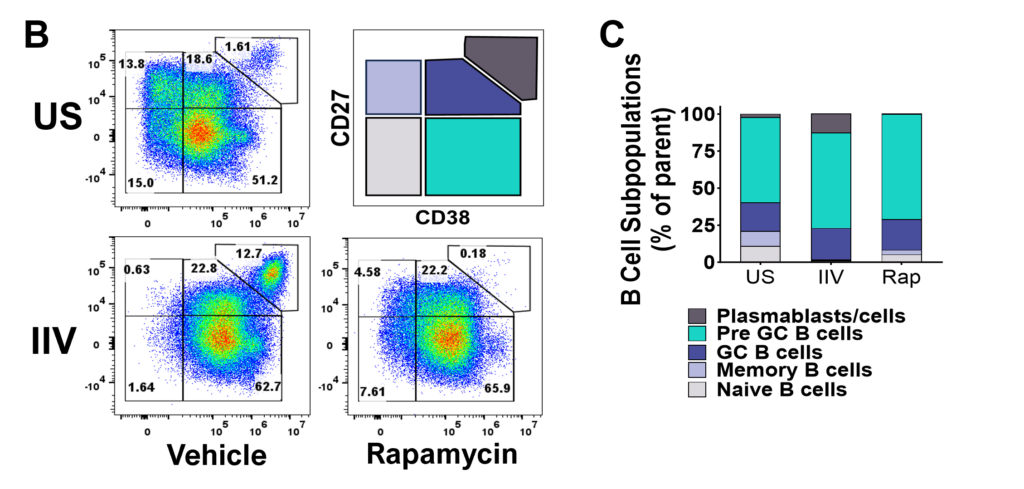
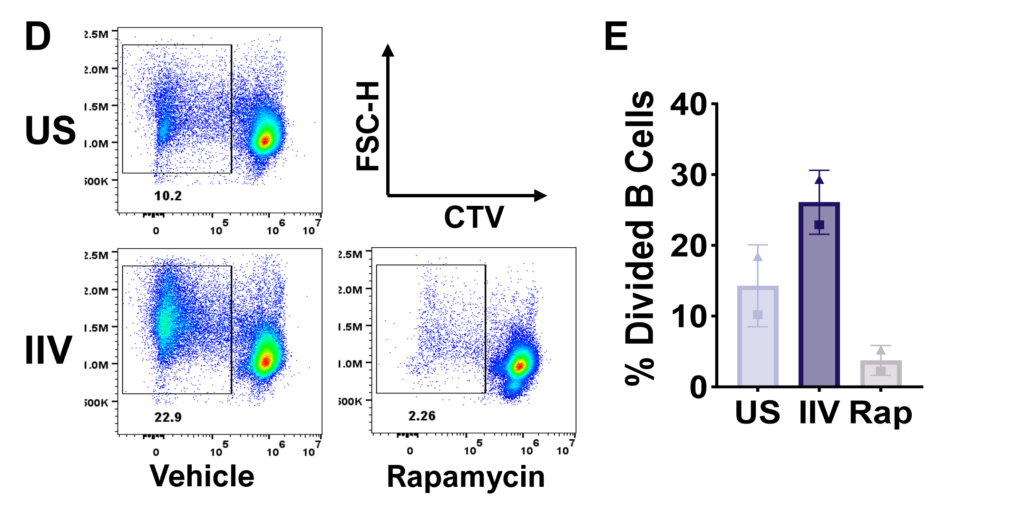
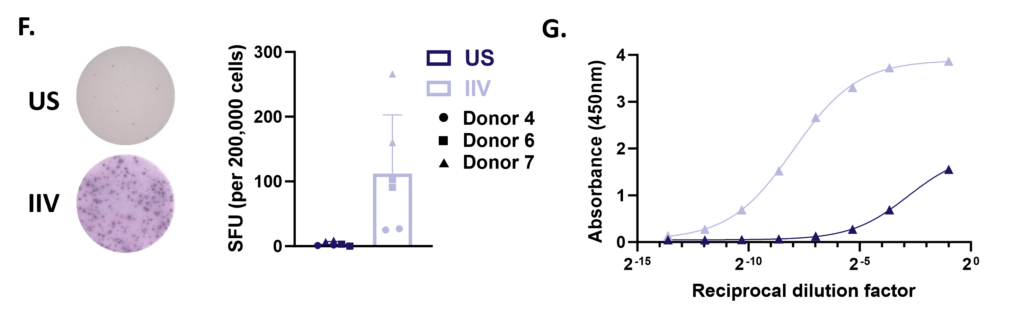
Figure F. HA-specific IgG production on day 7 measured by ELISpot. Representative images from one donor (left) and bar graph showing spot forming units (SFU) per 200,000 cells from 3 pre-selected IIV responsive donors run in duplicate wells (right). G. HA-specific IgG secretion on day 12 by ELISA. Representative dilution curves from one donor
Peripheral blood B cells can be stimulated with T-independent and T-dependent stimuli driving effector functions such as B cell activation, proliferation, Ig production and Ig class switching. Therapeutic intervention using pan or B cell suppressants – Rapamycin, Cyclosporin A or BTK inhibitor Ibrutinib respectively modify B cell function. Other B cell readouts such as downstream signaling following BcR cross linking and B cell antigen presentation to T cells can be assessed.
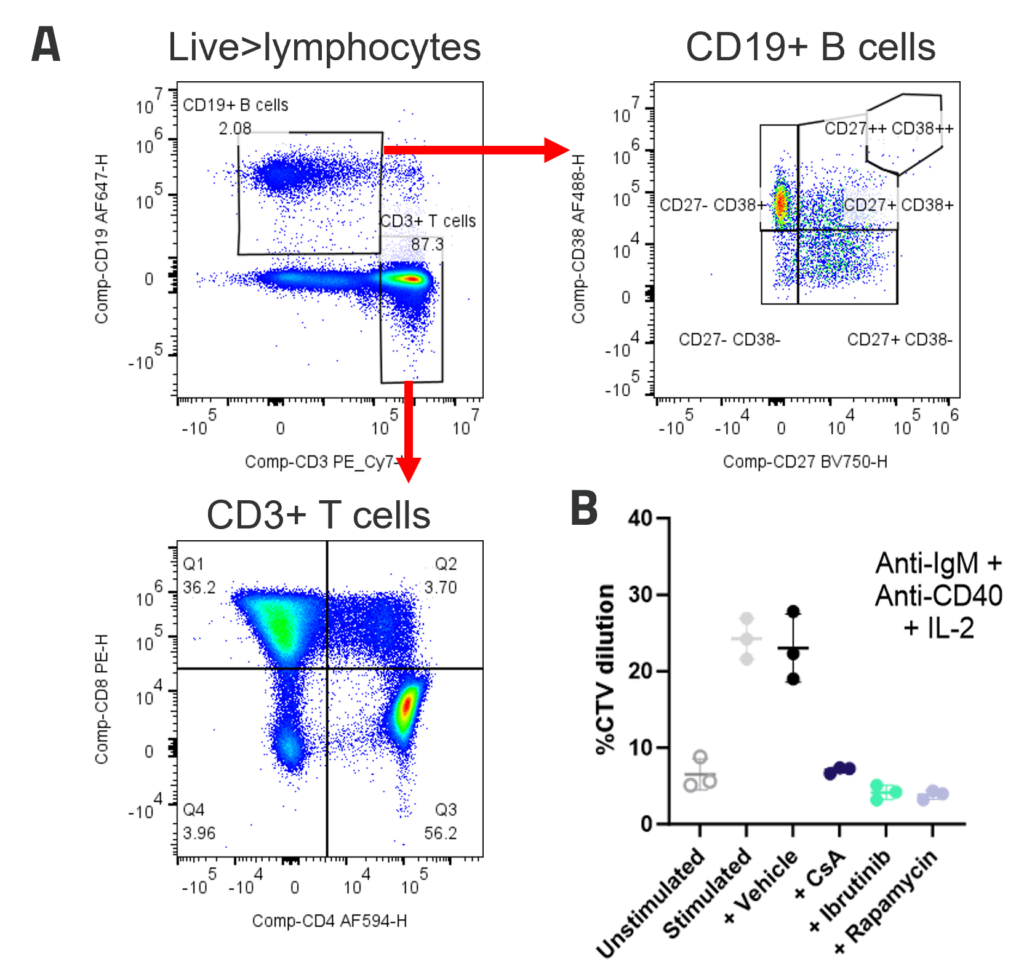
A. Peripheral blood B cells constitute around 2-5% of PBMC and contain predominantly naïve (CD27-CD38+) and memory (CD27+CD38-) populations. Example B and T cell profiles in unstimulated PBMC (B) B cell proliferation to polyclonal T dependent stimuli. PBMC were stimulated with anti-IgM + anti-CD40+ IL-2. Graphs show B cell %CTV dilution as a measure of proliferation Stimulation was performed in the presence or absence of inhibitors; FK506, Ibrutinib or Rapamycin. Bars indicate mean +/- SD, n = 3 donors.
B cell depletion is reported to not only have the potential to alter levels of auto-antibodies but also the immune milieu – B cells produce many soluble mediators which impact on other immune cell types such as T cells and DC, so depletion of B cells has the potential to regulate other subsets involved in the disease process. Alemtuzumab was used to show NK cell mediated B cell depletion further examples using Rituximab are available.
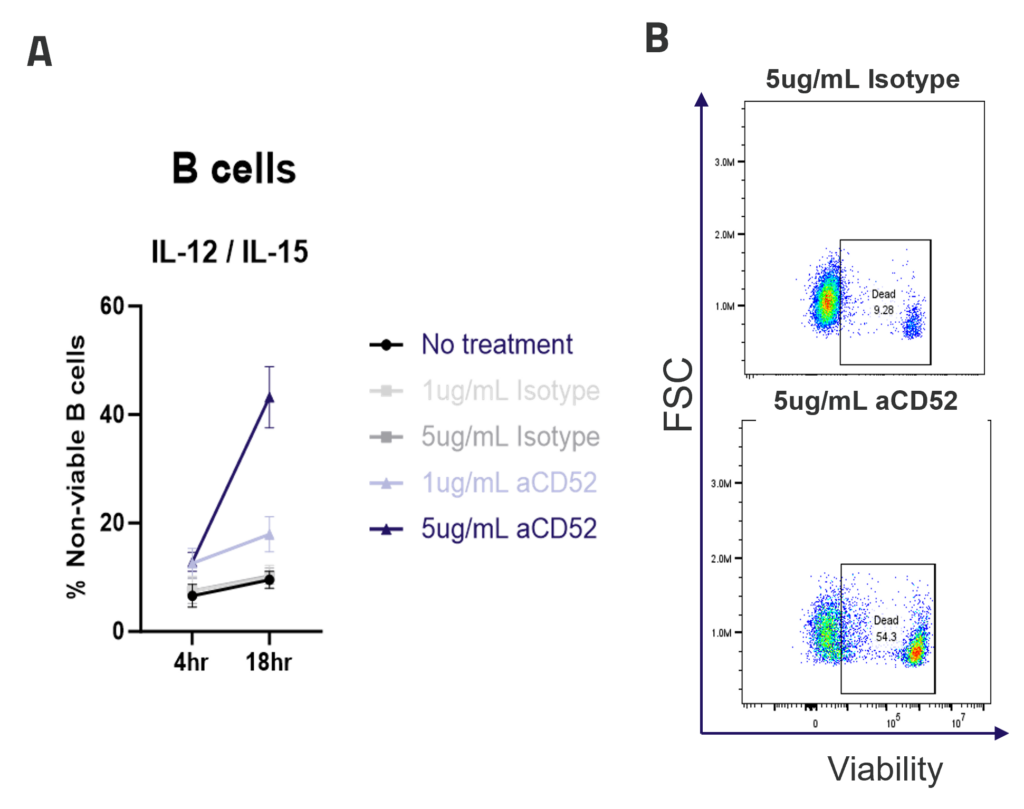
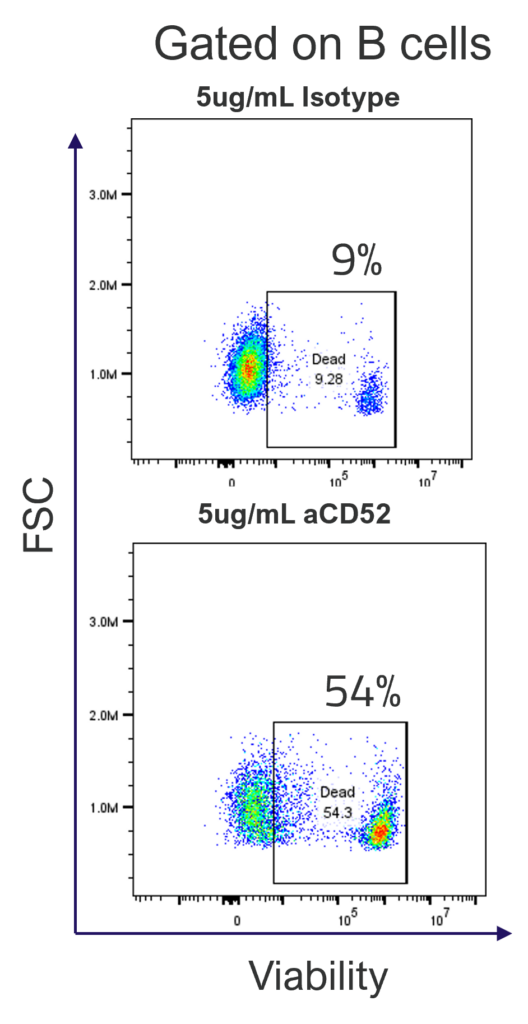
A. ADCC mediated B cell depletion. PBMCs were rested overnight with IL-12/IL-15 pre-activation, before addition of IgG1 isotype control or anti-CD52 Alemtuzumab (1ug/mL, 5ug/mL). The viability of CD4, CD8 and B cells (A) was measured by flow cytometry after 4 or 18hr of culture. Graphs show mean +/- SEM, n = 3 donors. Representative dot plots (B) show B cell viability after 18hr of culture.
CD4+ T cell
Immune-Oncology Assays
- Polyclonal
- MLR
- Antigen specificity
- nTreg suppression assay
- iTreg polarisation assay
Autoimmunity Assays
- Th1/2/17 polarisation
- Th17 function
- Tr1/iTreg polarisation
- nTreg suppression
- Tfh, naïve
- CM and EM phenotype/function
- Polyclonal T cell proliferation
- Cytokine release
Inflammation Assays
- Cytokine release
Assays
Enzyme-Linked Immuno Spot (ELISpot) enables quantification of rare immune cell function in response to antigenic stimulation
ELISpot is a highly sensitive method to test immune modulators, novel vaccine candidates or de-risk immunogenicity testing in an antigen-specific CD4 and/or CD8 T cell assay.
| Condition | Aim |
| No Stimulation | Negative control |
| PMA | Positive control |
| CERI (CMV, EBV, RSV, Influenza) | MHC-I restricted peptide pool to evaluate modulation of CD8+ T-cell memory response |
| CPI (CMV, Parainfluenza, Influenza) | Positive protein antigens to evaluate modulation of CD4+ T-cell memory response |
| CEF (CMV, EBV, Influenza) | MHC-I restricted peptide pool to evaluate modulation of CD8+ T-cell memory response |
| Cyclosporin A (CsA) | Inhibition of immune response |
Figure 1: The ELISpot visual image results showing four donors under four conditions: Unstimulated (negative control), stimulated with PMA (positive control), stimulated with CERI, and stimulated with CPI antigens. Each purple spot represents one IFNγ producing cell.
Spot Forming Units (SPU) for IFN-γ per 100,000 PBMC from CERI, CPI and CEF antigens for three donors
Figure 2: T cell responses from three donors using stimuli, CERI (I), CPI (II) and CEF (III). Expressed as spot forming units per 100,000 donor PBMC. Depletion of CD4 or CD8 T cells demonstrates specificity of response to peptide pools. Each value represents the mean of triplicate wells ±SEM.
T helper 17 (Th17) cells, are a subset of CD4 T cells distinguished by their production of IL-17. While crucial for protecting the body against extracellular pathogens, Th17 cells have also been implicated in autoimmune disease. Discovering therapies that target either the differentiation or effector function of Th17 cells could therefore prove beneficial for the treatment of some autoimmune diseases.
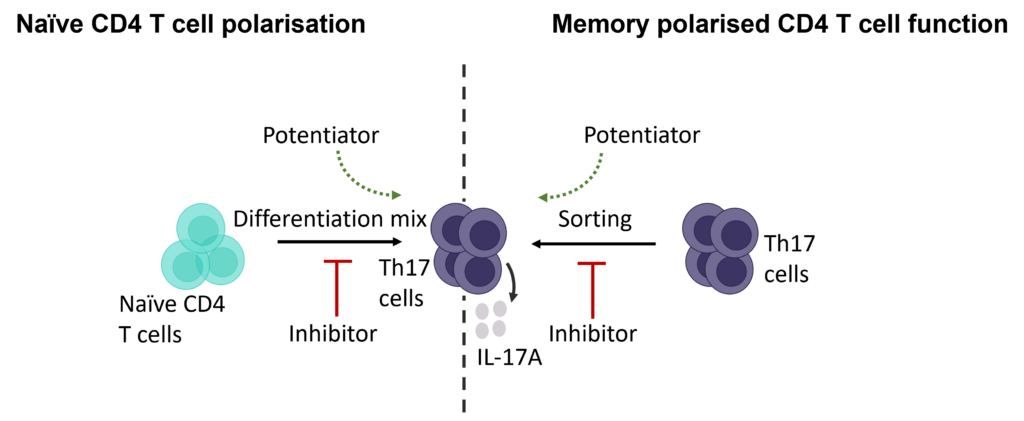
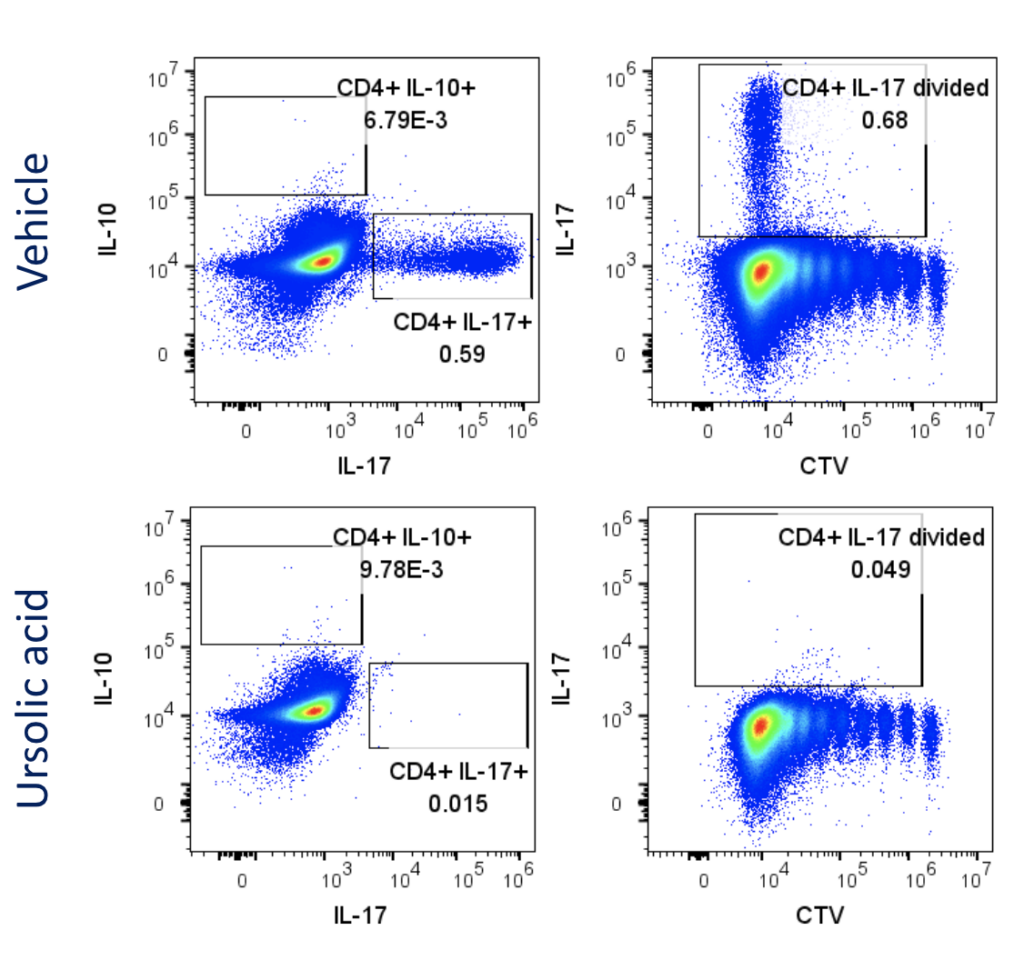
Evaluation of therapeutic modulation of Th17 differentiation
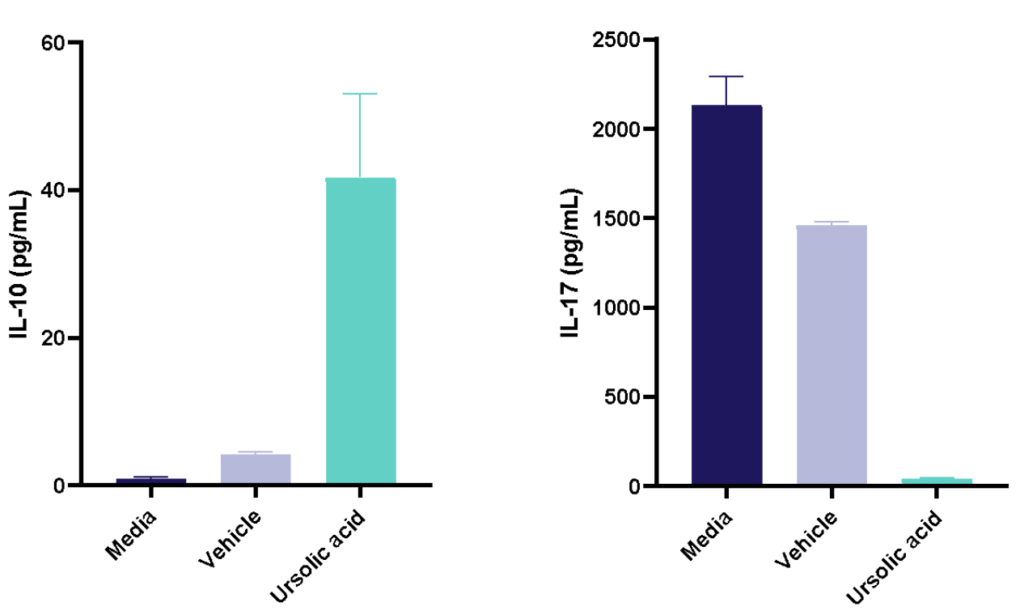
Figure 1: Polarisation of Th17 cells. Naïve CD4 cells were cultured under Th17 polarising conditions for 12 days in the presence or absence of Ursolic Acid. CD4 T cells were assessed for proliferation by CTV dilution; intracellular cytokine staining (ICS) of IL-17 and IL-10 by flow cytometry. On Day 12, Supernatants were collected and evaluated for IL-17 and IL-10 levels by MSD. RoRγT inhibitor Ursolic Acid showed selective inhibition of IL-17 production by intracellular cytokine staining (ICS) and MSD.
Evaluation of therapeutic modulation of Th17 effector function
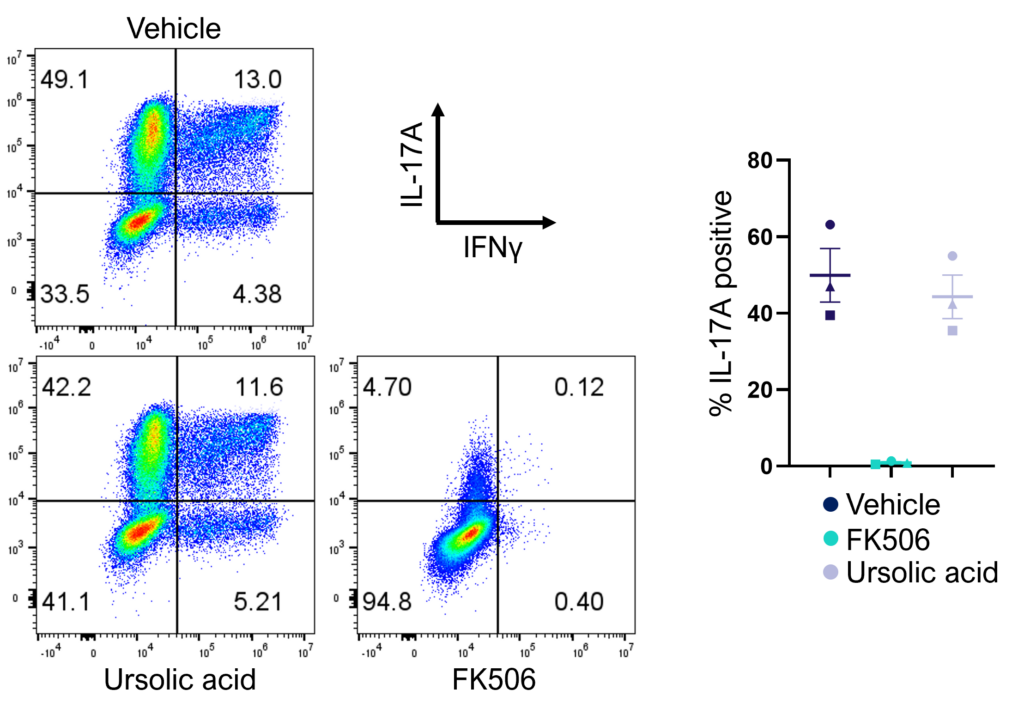
Figure 2: Inhibition of Th17 cell effector function. Magnetically sorted memory Th17 cells were polyclonally stimulated under Th17 conditions in the presence or absence of ursolic acid or FK506 for 5 days. A percentage of Th17 cells are polyfunctional (IL- 17A+IFNγ+) and refractory to inhibition by ursolic acid (an inhibitor of Th17 differentiation) but not FK506.
For many the humble “workhorse” mixed lymphocyte reaction (MLR) is a key screening assay for immuno-therapeutics. 1-way (DC and T cells) and 2-way MLRs (PBMC) provide expression of key ligands on human immune cells for therapeutic modulation.
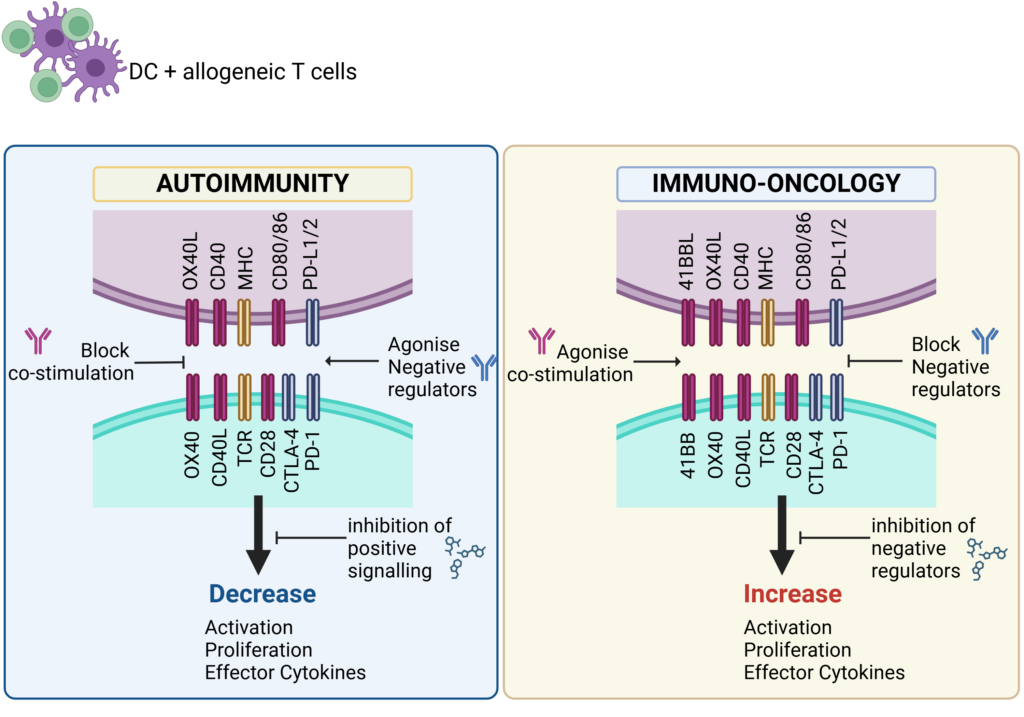
Schematic showing key therapeutic targets that are blocked (antagonise) or engaged (agonise) to control immune responses in Autoimmunity or boost immune responses for Immuno-Oncology.
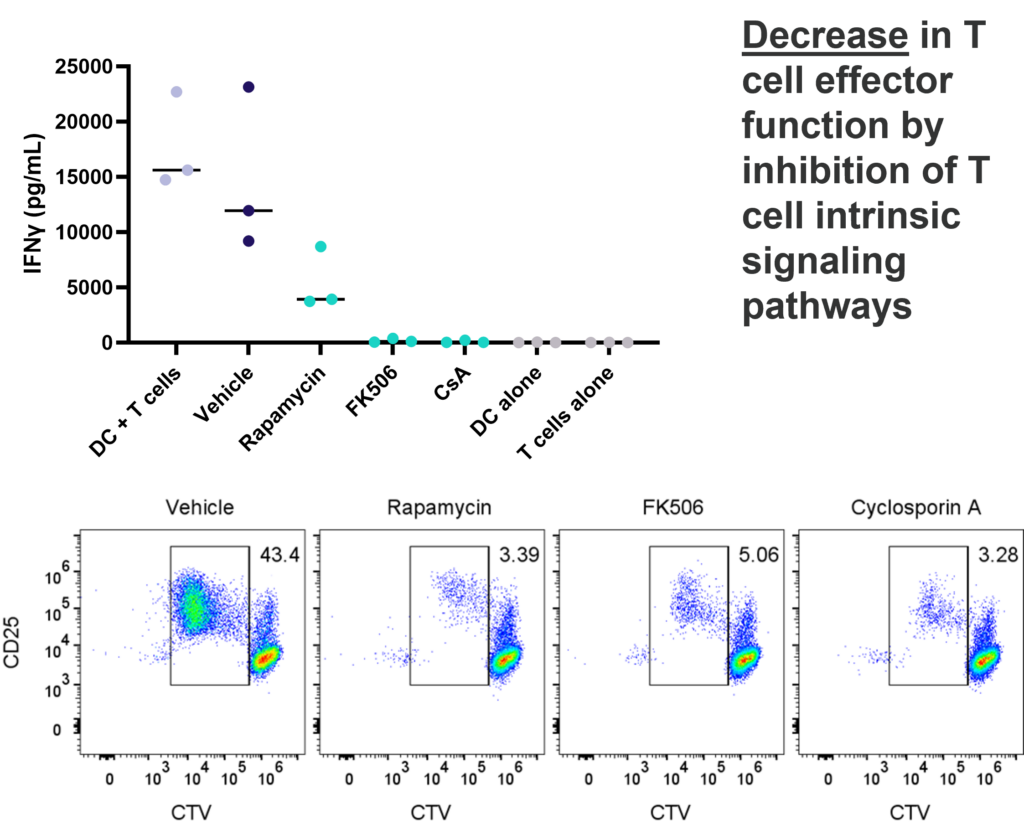
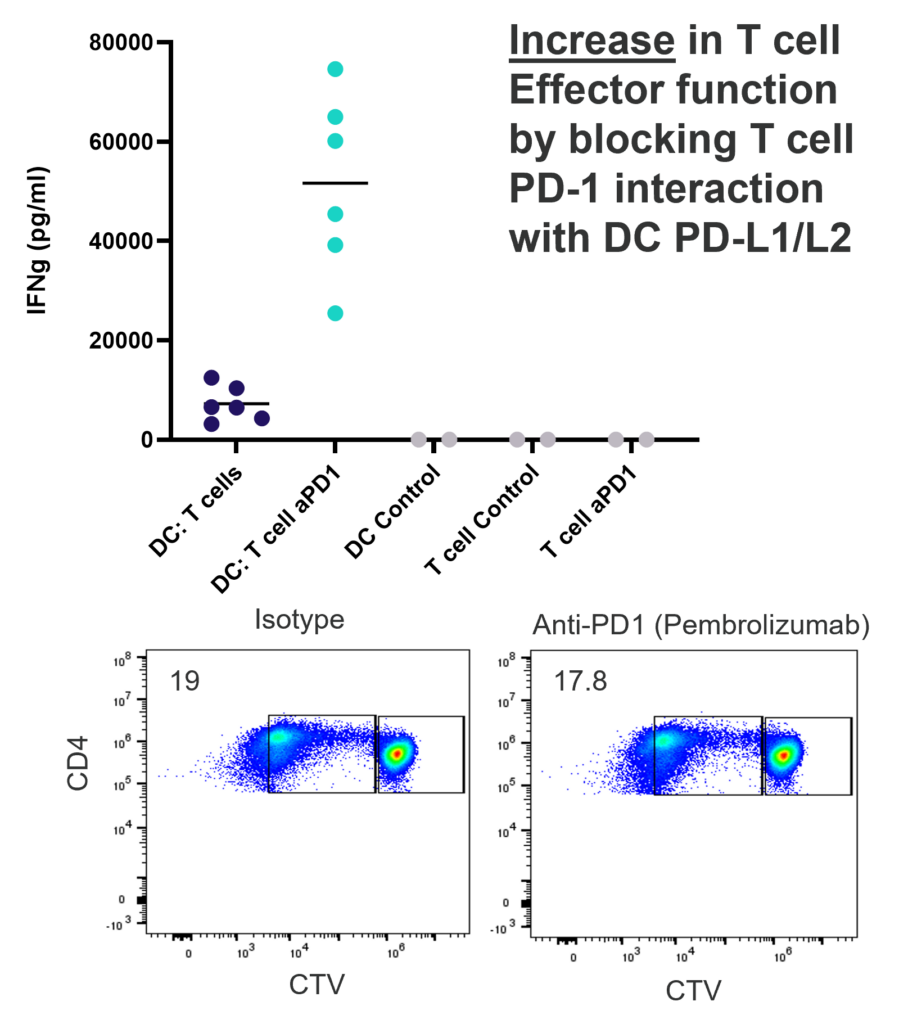
1-way or 2-way MLR. One way MLR of CTV labelled T cells in response to allogenic DC, matured with LPS. T cell proliferation and IFNγ production is inhibited by Rapamycin, FK506 and Cyclosporin A, in contrast, PD-1 blockade (Pembrolizumab) increases T cell IFNγ production, but does not enhance T cell proliferation.
This assay provides a relevant human system to test novel therapeutics that block or engage key co-stimulatory or inhibitory ligands expressed on immune cells.
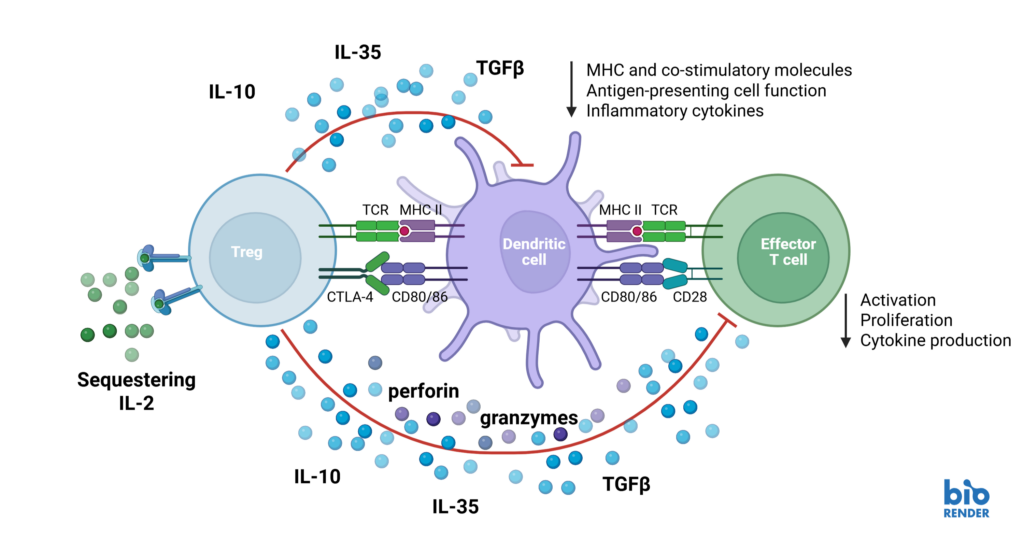
Natural Tregs (nTregs) are a thymus-derived subset of CD4+ T cells found in peripheral blood, capable of suppressing immune responses to maintain tolerance and homeostasis. Suppression assays model Treg function by measuring their ability to inhibit effector T cell proliferation, activation, and cytokine production. Altering Treg suppressive function can have promising therapeutic potential, both in the context of autoimmunity and immuno-oncology.
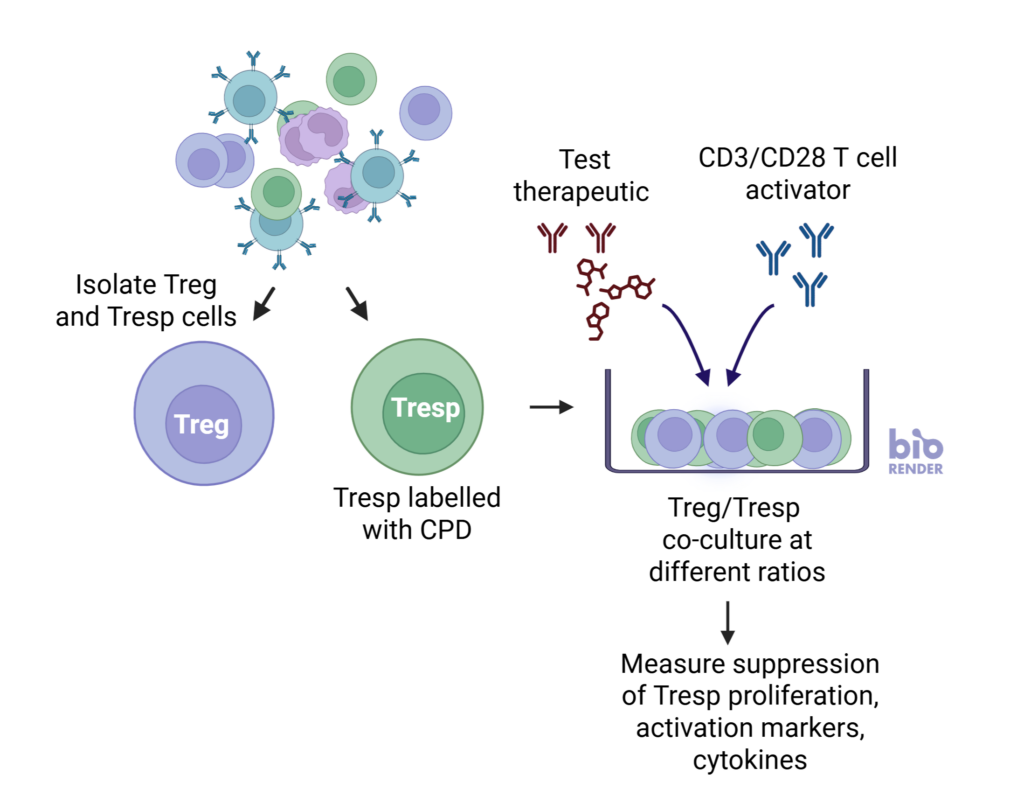
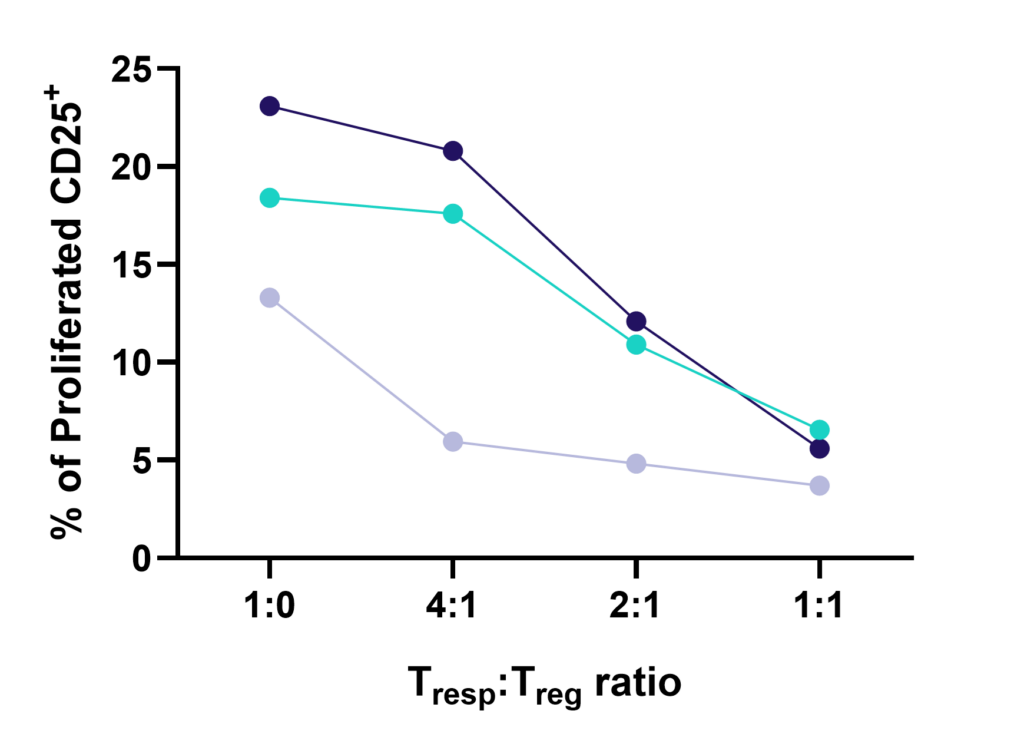
nTreg cells suppress the proliferation of Tresp cells in a ratio-dependent manner
nTregs were co-cultured with stimulated CD3 T cells at three Tresp:Treg ratios. Graphs show increased suppression of Tresponder proliferation in the presence of increasing number of Tregs. Data shown from three healthy donors.
I. T cell response to Tetanus Toxoid, Influenza and PPD antigens
II. Dose response to Influenza antigen
Antigen specific T cells response to a recall antigens. (I) Healthy donors PBMC were stimulated with PHA-M or triple antigen cocktail (Tetanus Toxoid, Influenza and PPD). Cyclosporin was used as a reference treatment. (II) Dose response to Influenza antigen. CD4 and CD8 T cells proliferation was measured by flow cytometry using CTV dilutions.
Cancer cell
Immune-Oncology Assays
- Immunogenic Cell Death
- 2D/3D Tumour Killing Assays (panel of tumour cells available)
- On/off target assay
- CDC
Assays
Figure 1: SKOV-3 NLR tumour cells were seeded into 96 well plates, PBMC were added once spheroids were established in the presence of Pembrolizumab or IgG4 control or vehicle (untreated) and imaged every 4 hours for 96 hours using the CellCyte X. Relative spheroid area (%) was measured (A). AUC statistics were calculated using GraphPad Prism v9.5.0
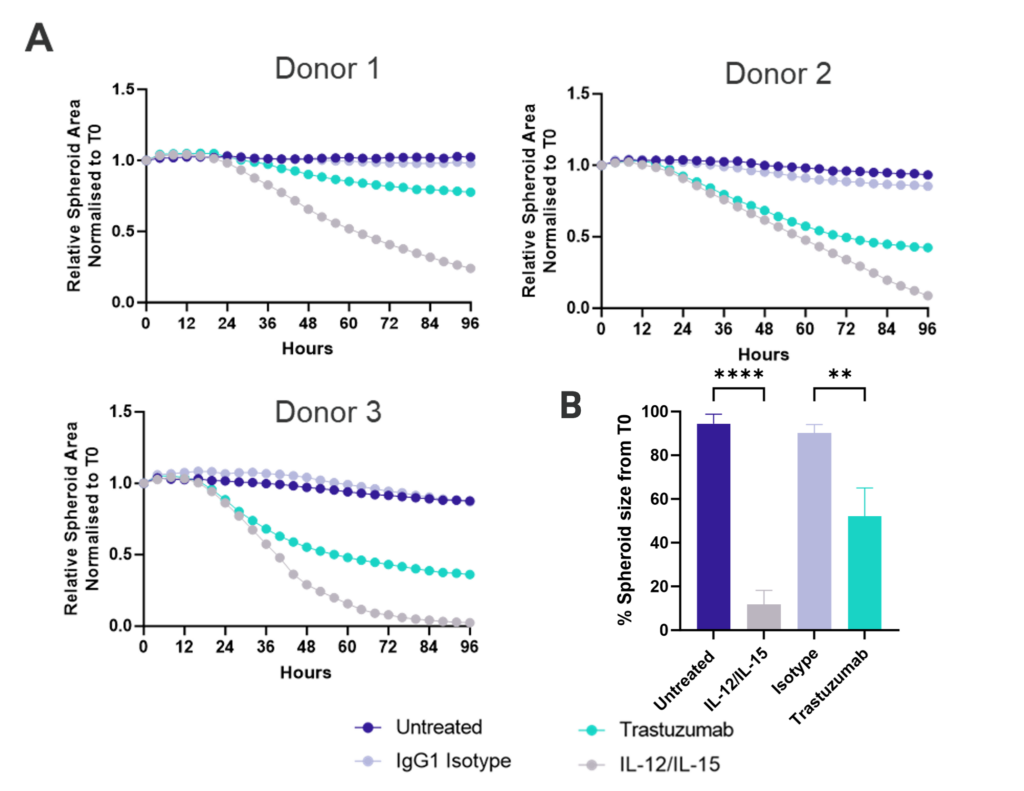
Figure 1: SK-OV-3 NLR cells expressing HER2 were plated were seeded into 96 well plates and once spheroids were established purified NK cells were added to cultures in the presence of Trastuzumab or IgG1 Isotype or IL-12/IL-15 or vehicle (untreated) and imaged every 4 hours for 96 hours using the CellCyte X. Relative spheroid area (%) was measured (A) and the AUC (B) calculated using GraphPad Prism v9.5.0. Line graphs show the mean of triplicate wells and the bar graph shows mean +/- SEM of 9 donors. (C) Representative images from the CellCyte X at 96 hours post NK cell addition to tumour spheroids.
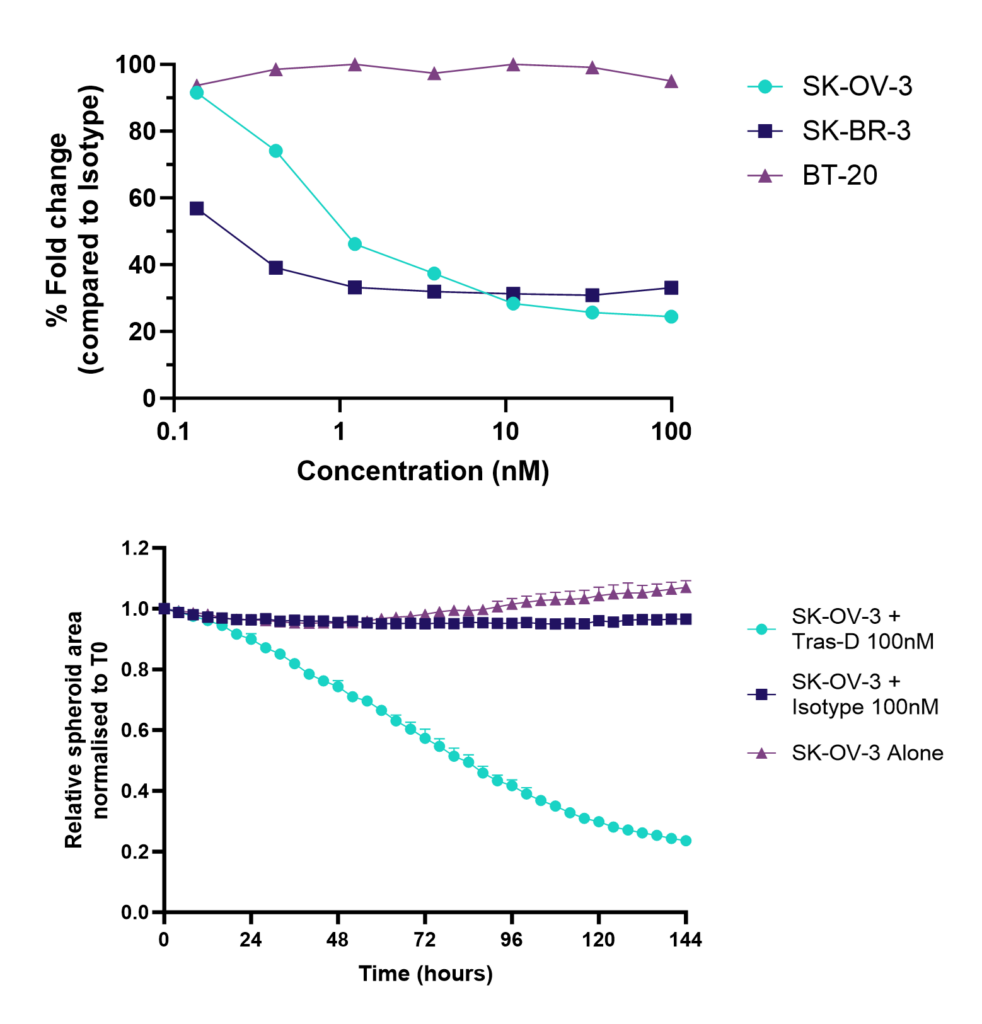
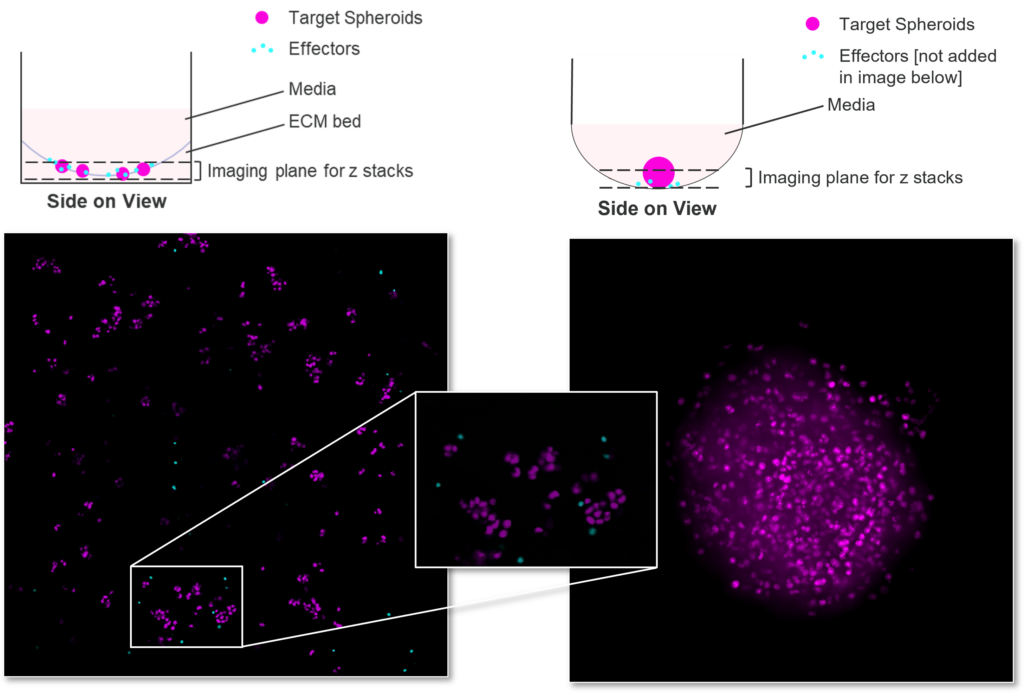
Figure 1: SK-OV-3, SK-BR-3 and BT-20 NLR cells were seeded into 96 well plates; Trastuzumab-Deruxtecan or Isotype control was added once spheroids were established and imaged every 4 hours for 96 hours using the CellCyte X. Data shows tumour cytotoxicity normalised to isotype control, and example killing kinetics.
Monocyte
Inflammation Assays
Assays
Inflammasomes are key signaling platforms within the immune system. Inflammasome complexes form in response to infection, tissue damage or metabolic imbalances. Once formed the inflammasomes activate Caspase 1 which in turn activated the pro-inflammatory cytokines IL-1β and IL-18. Targeting the inflammasome and the resulting signaling pathways is a useful tool in modulating the immune system.
Effect of MCC950 on Inflammasome activation – IL-1β and IL-18.
PBMC from three healthy donors were pretreated with MCC950, vehicle (DMSO) or media for 1 hours prior to stimulation with LPS for 4 hours. Nigericin was then added for a further 45 minutes prior to harvest of the cell culture supernatant for quantification of (A) IL-1β and (B) IL-18 by TR-FRET and ELISA respectively. Data points show mean +/- SEM of technical replicates. One-way ANOVA with Dunnett’s multiple comparisons test comparing stimulated (media) to unstimulated, LPS alone, vehicle and MCC950 to vehicle; *<0.05, **<0.01, ***<0.001.
Other formats: PBMC, macrophage subsets, microglia
Cytokine release assay can be used to “de-risk” any potential unwanted effects of novel biotherapeutics in accordance with FDA and EMA recommended guidelines.
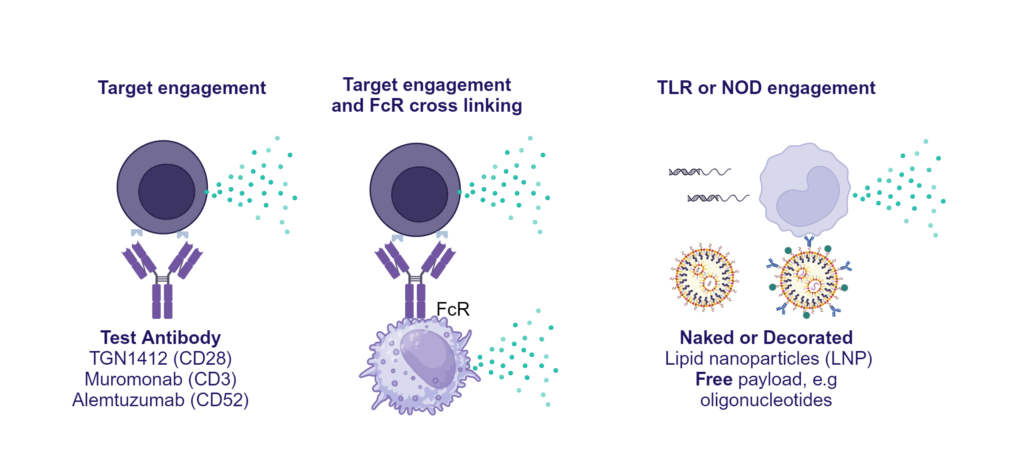
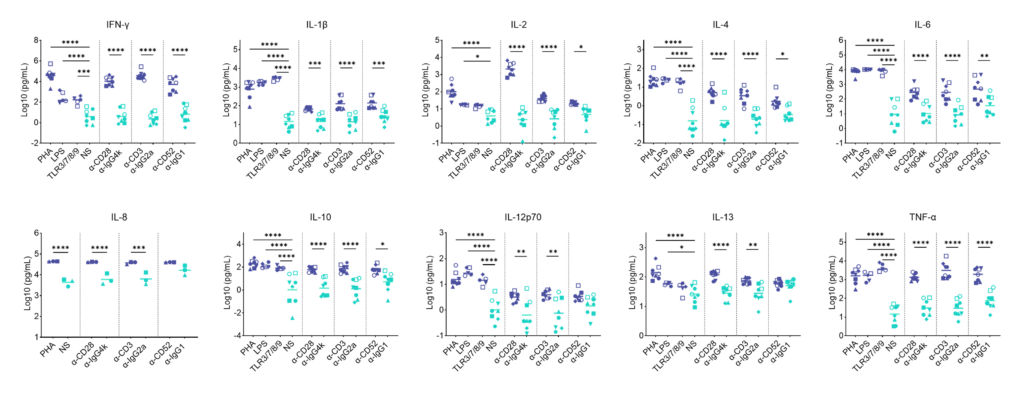
Preclinical safety PBMC cytokine release assay (CRA)
PBMC solid phase CRA: release of IFN-γ, IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, IL-12p70, IL-13 and TNF-α in response to a panel of antibodies coated onto plastic or TLR stimuli or polyclonal T cell stimuli (PHA).
PBMC isolated from buffy coats were added to wells coated with a-CD28 (TGN1412), a-CD3 (Muromonab), a-CD52 (Alemtuzumab) or with isotype control antibodies, or were stimulated with PHA, LPS, or a cocktail of TLR3/7/8/9 agonists. Cytokine release was measured at 48hr post stimulation. NS = Non-stimulated; Graphs show log10 transformed data with mean of 10 donors indicated. One way ANOVA with Sidak’s multiple comparisons test performed on log10 transformed data with significance indicted as *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001. Note for IL-8 where values were above the ULOD these were assigned ULOD value.
Other readouts: frozen disease PBMC
Other formats: Whole Blood CRA
Other immuno-tox assays: include ADCC/ CDC/ ADCP
Preclinical safety whole blood cytokine release assay (CRA)
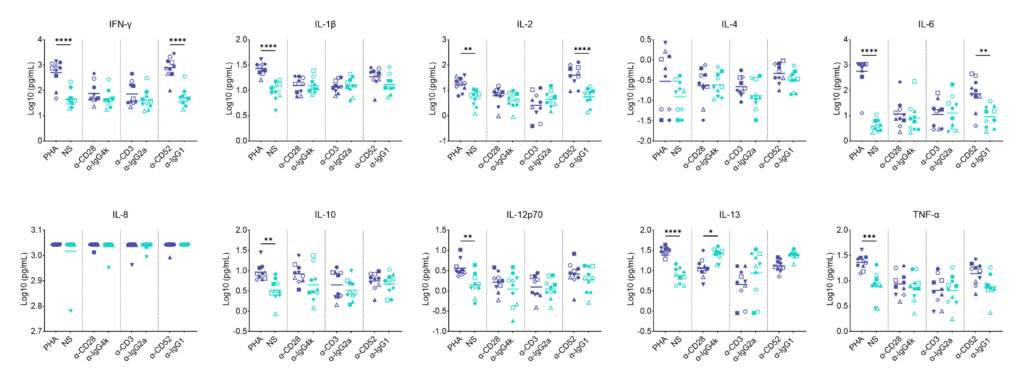
Whole blood soluble CRA; release of IFN-γ, IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, IL-12p70, IL-13 and TNF-α in response to a panel of antibodies or polyclonal T cell stimuli (PHA).
Whole blood was added to wells containing a-CD28 (TGN1412), a-CD3 (Muromonab), a-CD52 (Alemtuzumab) or with isotype control antibodies or were stimulated with PHA. Cytokine release was measured at 48hr post stimulation by MSD. NS = Not stimulated. Graphs show log10 transformed data with mean of 10 donors indicated. One way ANOVA with Sidak’s multiple comparisons test performed on log10 transformed data with significance indicted as *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001. Note for IL-8 where values were above the ULOD these were assigned the ULOD value.